Download to read offline

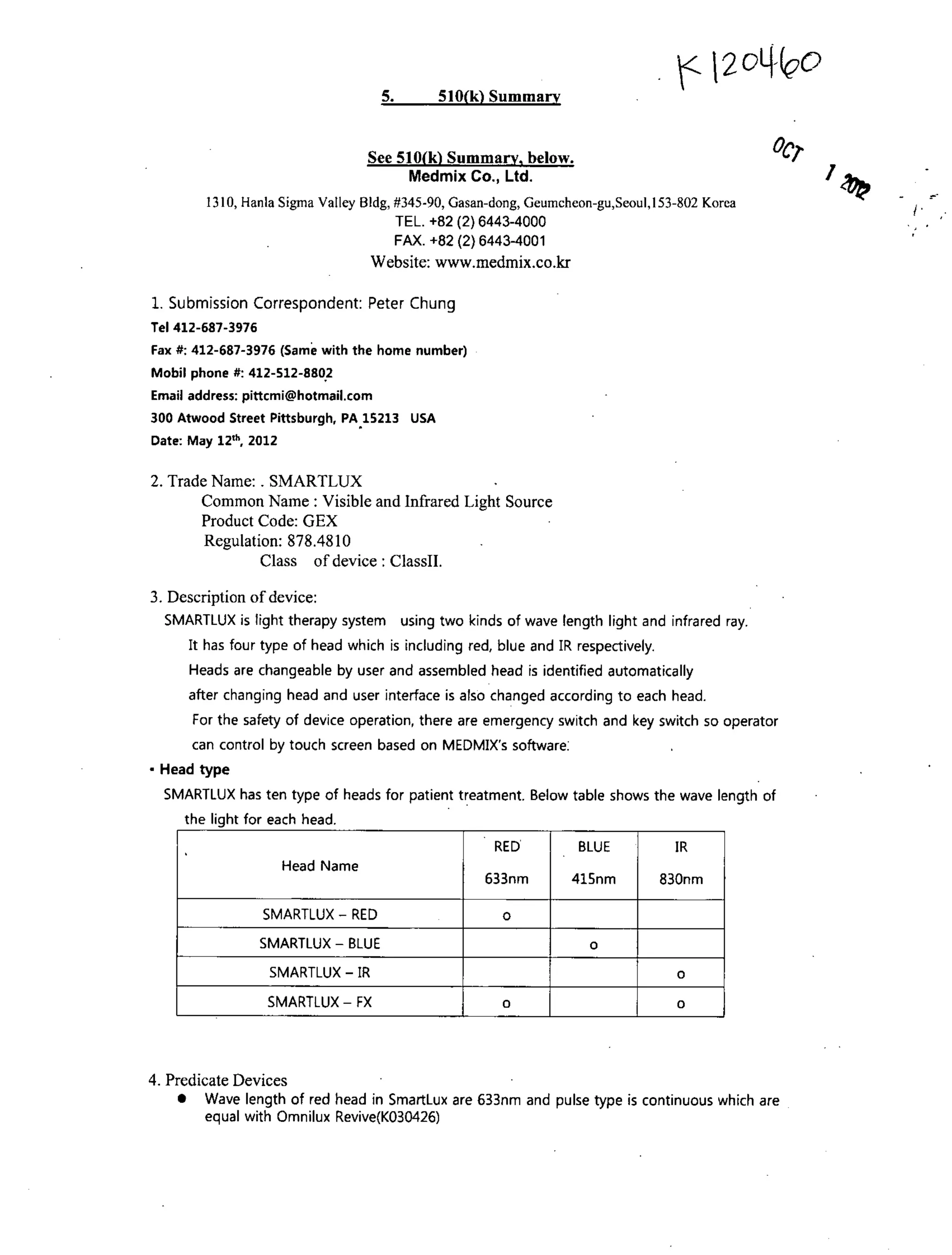
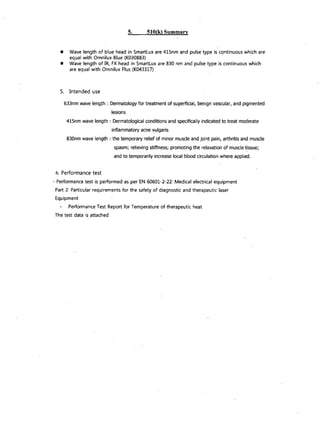
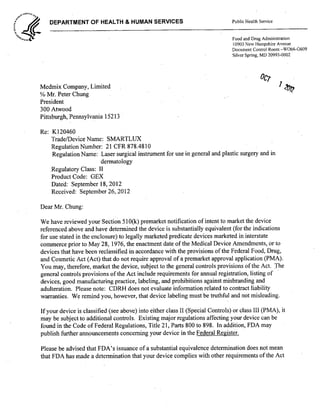

This document summarizes a 510(k) submission for a light therapy system called SMARTLUX. SMARTLUX uses red, blue, and infrared light from interchangeable heads to treat various dermatological and musculoskeletal conditions. Performance testing shows it is substantially equivalent to legally marketed predicate devices. The FDA found SMARTLUX to be substantially equivalent and can be marketed for treating superficial lesions with 633nm light, acne with 415nm light, and muscle/joint pain with 830nm light.















































![Disk Drill Pro 5.4.845.0 Crack With Activation Code [Latest 2025]](https://cdn.slidesharecdn.com/ss_thumbnails/manualbiomaglumina3deen231017dcompressed-250325121431-d13b6107-250401105331-e24f15b4-thumbnail.jpg?width=640&height=640&fit=bounds)














![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




