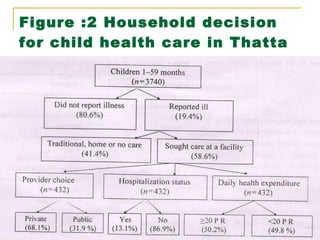
This study examined whether child gender determines household healthcare decisions in rural Thatta, Pakistan. The study found that while illness was reported more for infant girls, there was no significant difference in care seeking or healthcare expenditures between boys and girls. Girl children had higher mortality ratios than boys. The presence of a girl's school in a village was associated with lower rates of hospitalization, suggesting communities that value girls' education may also value their health more. Overall, the study found no evidence that households in Thatta differentially seek healthcare for boys over girls.
![Authors R. Nuruddin , Assistant Professor 1,2 W. C. Hadden , Visiting Faculty 1 , M. R. Petersen , Independent Consultant 3 M. K. Lim , Associate Professor 2 Department of Community Health Sciences, Aga Khan University , Stadium Road, PO Box 3500, Karachi 74800, Pakistan. Department of Community, Occupational and Family Medicine, Yong Loo Lin School of Medicine, National University of Singapore, 117597, Singapore. Independent Consultant, Cincinnati, Ohio, USA. Rozina Nuruddin , E-mail: [email_address]](https://image.slidesharecdn.com/jbfinal-100824045142-phpapp01/85/journal-club-3-320.jpg)