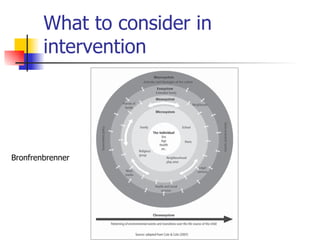
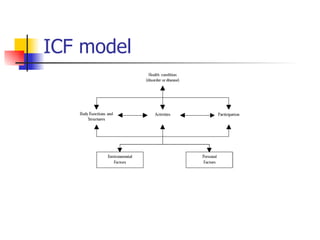
The document discusses various intervention approaches for children with developmental coordination disorder (DCD), highlighting both traditional 'bottom-up' and more effective 'top-down' task-specific strategies. It emphasizes the importance of functional, evidence-based interventions that involve families and take into account the child’s preferences and the contextual environment. Ultimately, it concludes that the most effective learning occurs through practice of relevant tasks and that interventions should focus on skills relevant to everyday life.









































![Odu%20 clinical%20science%20iii%20dcd%202011[1]](https://cdn.slidesharecdn.com/ss_thumbnails/odu20clinical20science20iii20dcd2020111-111213203143-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)













































