Definition
Definition
Infective endocarditisis microbial infection
of the endocardial surface of the heart
Commonly involves the valves
Characterised by formation of vegetation
that are composed of:
– Inflammatory cells
– Fibrin
– Platelets
May be classified as
– Acute or subacute
3.
aetiology
aetiology
Staphylococci
Staphylococci
– Commonestcause of endocarditis
Commonest cause of endocarditis
– S. aureus most common organism in cases of
S. aureus most common organism in cases of
right sided endocarditis in IV drug users and
right sided endocarditis in IV drug users and
HIV Positive Pt
HIV Positive Pt
– S. epidermidis common in prosthetic valves
S. epidermidis common in prosthetic valves
Streptococci
Streptococci
– S. viridans most common
S. viridans most common
– Enterococci occurring in elderly
Enterococci occurring in elderly
4.
Other causes
Othercauses
– Fungi-in intravenous drug users,
Fungi-in intravenous drug users,
immunocompromised patients
immunocompromised patients
– Gram negative bacilli
Gram negative bacilli
– Gonococcal
Gonococcal
– Pneumococcal
Pneumococcal
HACEK group
HACEK group
– Haemophilus
Haemophilus
– Actinobacillus
Actinobacillus
– Cardiobacterium
Cardiobacterium
– Eikenella
Eikenella
– kingella
kingella
Pathophysiology
Pathophysiology
normal endotheliumis resistant to
infection by most bacteria and to
thrombus formation
Infective endocarditis occurs at sites of
Infective endocarditis occurs at sites of
pre-existing endocardial damage
pre-existing endocardial damage
Organism may directly infect the Intact
endothelium or exposed subendothelial
tissue,
These areas attract fibrin and platelet
These areas attract fibrin and platelet
aggregation.
aggregation.
Platelet plugs further attract colonization
Platelet plugs further attract colonization
by microbial organisms
by microbial organisms
7.
Pathophysiology cont.d
Pathophysiology cont.d
Vegetations may grow
Vegetations may grow
Large vegetations
Large vegetations
– may break away as emboli
may break away as emboli
– May destroy adjacent tissues
May destroy adjacent tissues
– May cause aneurysm
May cause aneurysm
8.
Frequency of cardiac
Frequencyof cardiac
valve involvement
valve involvement
mitral>aortic>tricuspid>pulmonary
mitral>aortic>tricuspid>pulmonary
30% of patients have concomitant
30% of patients have concomitant
aortic and mitral valve involvement
aortic and mitral valve involvement
5% of patients have simultaneous
5% of patients have simultaneous
involvement of left and right sided
involvement of left and right sided
heart valves
heart valves
9.
Clinical features
Clinical features
Highly variable
Highly variable
Can be acute or subacute
Can be acute or subacute
Can be classed as
Can be classed as
– Native valve endocarditis
Native valve endocarditis
– Prosthetic valve endocarditis
Prosthetic valve endocarditis
– Endocarditis in intravenous drug users
Endocarditis in intravenous drug users
10.
Features continued
Features continued
Fever
Fever
– Generally present but may be absent in
Generally present but may be absent in
elderly or immunosuppressed
elderly or immunosuppressed
– In subacute endocarditis, fever is typically
low-grade and rarely exceeds 39.4C
Cardiac Manifestations
– Heart murmur
Heart murmur
– CCF in 30 to 40%
CCF in 30 to 40%
11.
Musculoskeletal
Musculoskeletal
– Painlesserythematous papule and
Painless erythematous papule and
macules in the palms and soles
macules in the palms and soles
– Painful erythematoue subcutaneous
Painful erythematoue subcutaneous
nodules in the pulp space of the fingers
nodules in the pulp space of the fingers
and toes
and toes
– Petechiae haemorrhages
Petechiae haemorrhages
– Splinter haemaorrhages
Splinter haemaorrhages
Splenomegaly
Splenomegaly
Flame shaped retinal haemorrhages
Flame shaped retinal haemorrhages
with pale centre-
with pale centre-ROTH SPOTS
ROTH SPOTS
investigations
investigations
Blood cultures
Bloodcultures
– Are positive in 85 to 90% of pt
Are positive in 85 to 90% of pt
– Collect up to 6 specimens
Collect up to 6 specimens
Echocardiogram
Echocardiogram
– Useful to demonstrate vegetations
Useful to demonstrate vegetations
– And evaluate valvular damage and
And evaluate valvular damage and
ventricular function
ventricular function
Major complications of
Majorcomplications of
endocarditis
endocarditis
Congestive heart failure
Congestive heart failure
Embolism
Embolism
– CNS-leads to CVAs, Seizure disorders,
CNS-leads to CVAs, Seizure disorders,
brain abscess
brain abscess
– KIDNEYS-may manifest with
KIDNEYS-may manifest with
haematuria
haematuria
– SPLEEN- splenic infarcts
SPLEEN- splenic infarcts
17.
Management
Management
Two aspects
Twoaspects
– Medical and
Medical and
– Surgical management.
Surgical management.
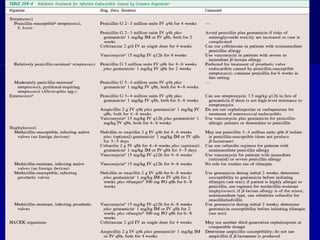
Medical management
Medical management
– Antibiotic therapy should be commenced
Antibiotic therapy should be commenced
– Aim the initial antibiotic therapy at the
Aim the initial antibiotic therapy at the
most likely cause.
most likely cause.
19.
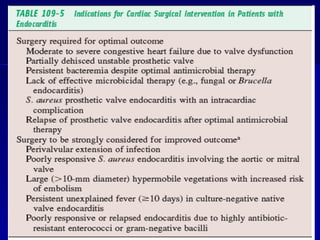
Surgical treatment
Surgicaltreatment
– Indications for cardiac surgery in pt
Indications for cardiac surgery in pt
with endocarditis include
with endocarditis include
Moderate to severe heart failure with valve
Moderate to severe heart failure with valve
dysfucntion
dysfucntion
Fungal endocarditis
Fungal endocarditis
21.
Prophylaxis
Prophylaxis
Cardiac conditionsfor which
Cardiac conditions for which
prophylaxis is indicated include
prophylaxis is indicated include
– High risk
High risk
– And low risk factors
And low risk factors






![Infective Endocarditis Group [A7] Seminar](https://cdn.slidesharecdn.com/ss_thumbnails/infectiveendocarditisa7-250627114414-bb3356a5-thumbnail.jpg?width=640&height=640&fit=bounds)





























































