Definition
• Infective endocarditisis microbial infection of the
endocardial surface of the heart
• Commonly involves the valves
• Characterised by formation of vegetation that are
composed of:
– Inflammatory cells
– Fibrin
– Platelets
• May be classified as
– Acute or subacute
3.
aetiology
• Staphylococci
– Commonestcause of endocarditis
– S. aureus most common organism in cases of right sided
endocarditis in IV drug users and HIV Positive Pt
– S. epidermidis common in prosthetic valves
• Streptococci
– S. viridans most common
– Enterococci occurring in elderly
4.
• Other causes
–Fungi-in intravenous drug users, immunocompromised
patients
– Gram negative bacilli
– Gonococcal
– Pneumococcal
• HACEK group
– Haemophilus
– Actinobacillus
– Cardiobacterium
– Eikenella
– kingella
Pathophysiology
• normal endotheliumis resistant to infection by
most bacteria and to thrombus formation
• Infective endocarditis occurs at sites of pre-
existing endocardial damage
• Organism may directly infect the Intact
endothelium or exposed subendothelial tissue,
• These areas attract fibrin and platelet
aggregation.
• Platelet plugs further attract colonization by
micobial organisms
Frequency of cardiacvalve
involvement
• mitral>aortic>tricuspid>pulmonary
• 30% of patients have concomitant aortic and
mitral valve involvement
• 5% of patients have simultaneous
involvement of left and right sided heart
valves
9.
Clinical features
• Highlyvariable
• Can be acute or subacute
• Can be classed as
– Native valve endocarditis
– Prosthetic valve endocarditis
– Endocarditis in intravenous drug users
10.
Features continued
• Fever
–Generally present but may be absent in elderly or
immunosuppressed
– In subacute endocarditis, fever is typically low-
grade and rarely exceeds 39.4C
• Cardiac Manifestations
– Heart murmur
– CCF in 30 to 40%
11.
• Musculoskeletal
– Painlesserythematous papule and macules in
the palms and soles
– Painful erythematoue subcutaneous nodules
in the pulp space of the fingers and toes
– Petechiae haemorrhages
– Splinter haemaorrhages
• Splenomegaly
• Flame shaped retinal haemorrhages with
pale centre-ROTH SPOTS
investigations
• Blood cultures
–Are positive in 85 to 90% of pt
– Collect up to 6 specimens
• Echocardiogram
– Useful to demonstrate vegetations
– And evaluate valvular damage and ventricular
function
Major complications of
endocarditis
•Congestive heart failure
• Embolism
– CNS-leads to CVAs, Seizure disorders, brain
abscess
– KIDNEYS-may manifest with haematuria
– SPLEEN- splenic infarcts
17.
Management
• Two aspects
–Medical and
– Surgical management.
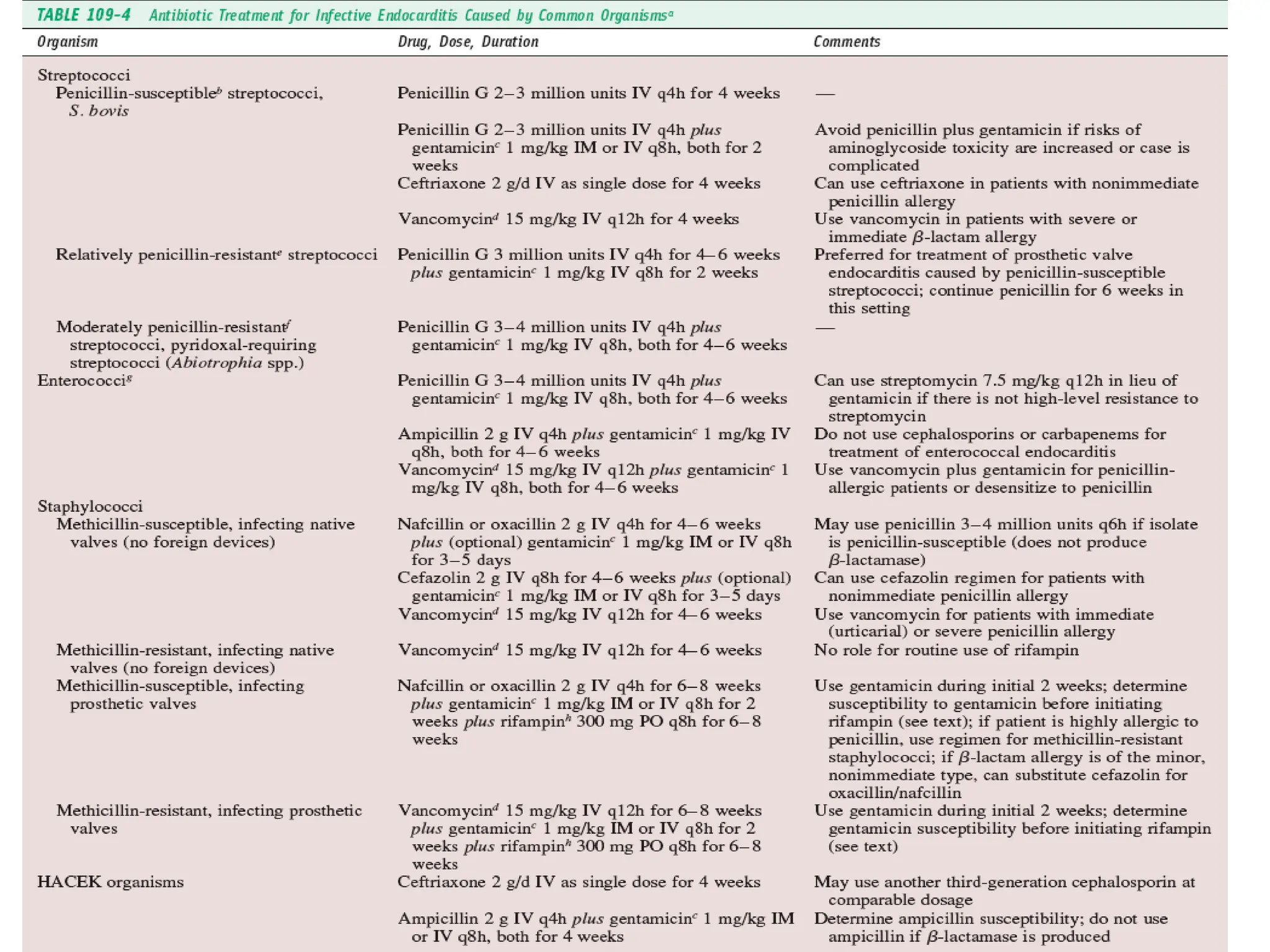
• Medical management
– Antibiotic therapy should be commenced
– Aim the initial antibiotic therapy at the most likely
cause.
19.
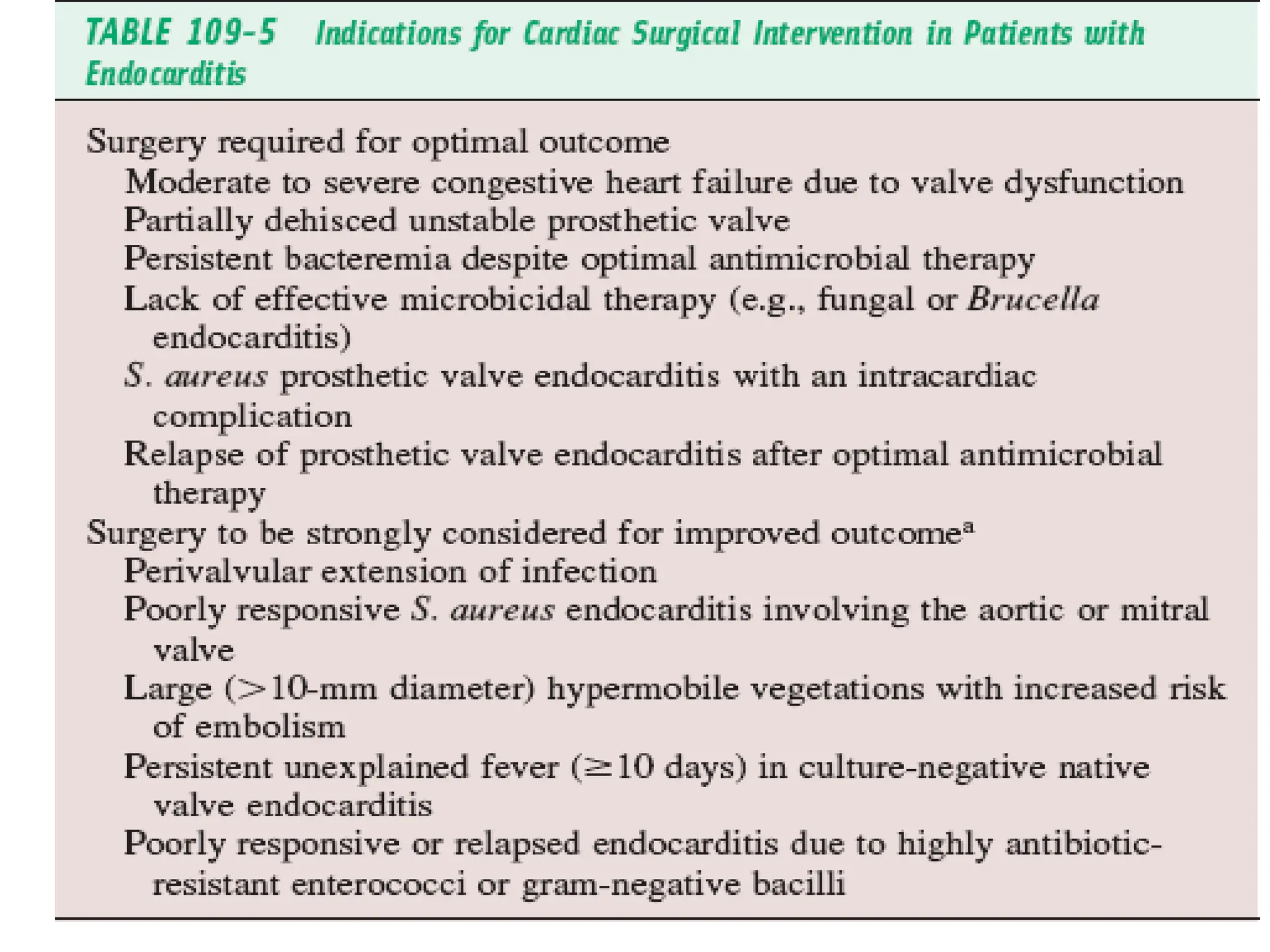
• Surgical treatment
–Indications for cardiac surgery in pt with
endocarditis include
• Moderate to severe heart failure with valve
dysfucntion
• Fungal endocarditis






















![Infective Endocarditis Group [A7] Seminar](https://cdn.slidesharecdn.com/ss_thumbnails/infectiveendocarditisa7-250627114414-bb3356a5-thumbnail.jpg?width=640&height=640&fit=bounds)












































