Download to read offline




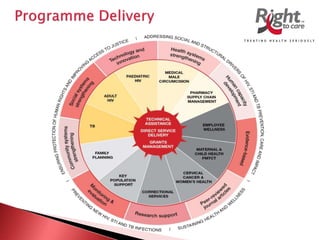
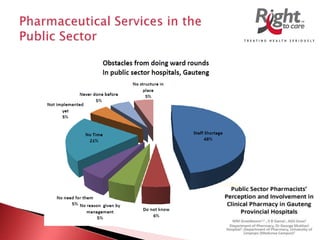

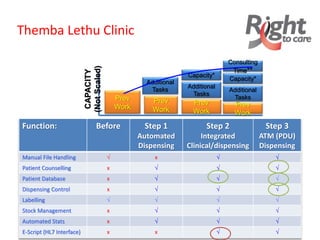
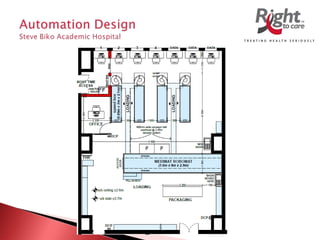

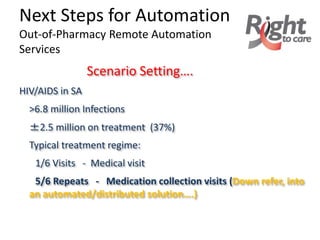



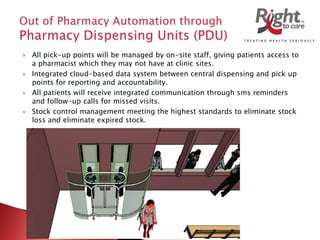
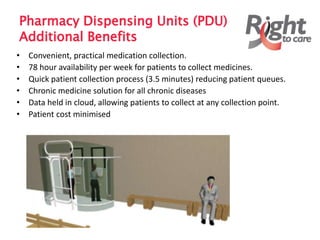
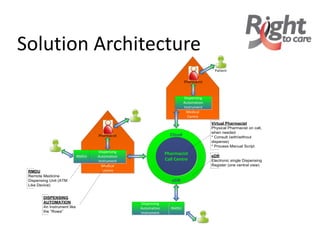




This document discusses an organization in South Africa that provides HIV/TB treatment and management services. Some key points: - The organization is a large non-profit founded in 2001 that supports government HIV/TB facilities and aims to improve treatment delivery. It receives international funding. - The document discusses challenges with pharmacy services and long wait times. It implemented an automation system at one hospital that led to reduced wait times, increased capacity, and improved stock management. - The organization aims to expand pharmacy automation and implement remote dispensing units to further improve access and efficiency of medication collection for chronic diseases like HIV/AIDS. It discusses regulatory considerations and plans to partner with government departments and international funders to scale up these services























































































