Inhalational injury refers to respiratory tract and systemic damage caused by inhalation of hot gases, steam or noxious combustion products. It affects 1/3 of burn admissions and significantly increases mortality, especially when combined with burns or pneumonia. Pathophysiology includes thermal damage, asphyxiation from carbon monoxide/cyanide, and pulmonary irritation leading to edema, inflammation and impaired function. Diagnosis is based on history, exam findings and investigations like ABGs, CXR and bronchoscopy. Management focuses on securing the airway, 100% oxygen, antibiotics for secondary infection, steroids and HBO for CO poisoning. Prognosis depends on severity of injury and presence of complications.


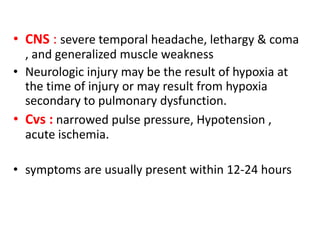
![ Arterial Blood Gases
• Hypoxia and hypercarbia in significant respiratory
distress .
• Arterial oxygen tension [PaO2] does not accurately
reflect the degree of CO poisoning or cellular
hypoxia , PaO2 level reflects the oxygen dissolved in
blood that is not altered by the hemoglobin-bound
CO
• Metabolic acidosis
• High (A-a) gradient
Cont.](https://image.slidesharecdn.com/inhalational-injury-2018-190403143310/85/Inhalational-injury-Dx-and-Tx-25-320.jpg)


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















