Downloaded 37 times



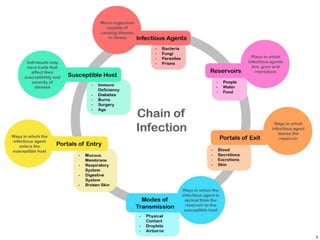






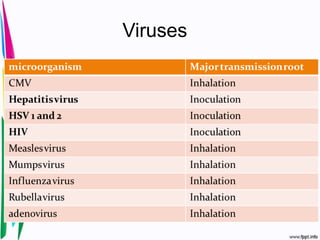
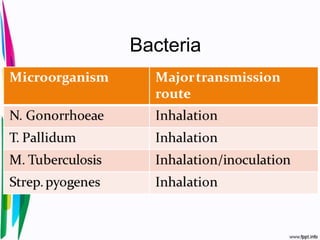







This document discusses infection control in dentistry. It begins by defining infection and infection control. It then discusses the history and objectives of infection control. The main modes of disease transmission in a dental setting are through airborne contamination, contact transmission, and cross-contamination. The document outlines various exposure risks for patients and dental personnel and infection control programs. It discusses sterilization and disinfection techniques as well as infectious diseases of concern in dentistry such as viral, bacterial, fungal, and parasitic infections. The principles of universal precautions like hand hygiene and protective barriers are emphasized.












































































