Downloaded 85 times
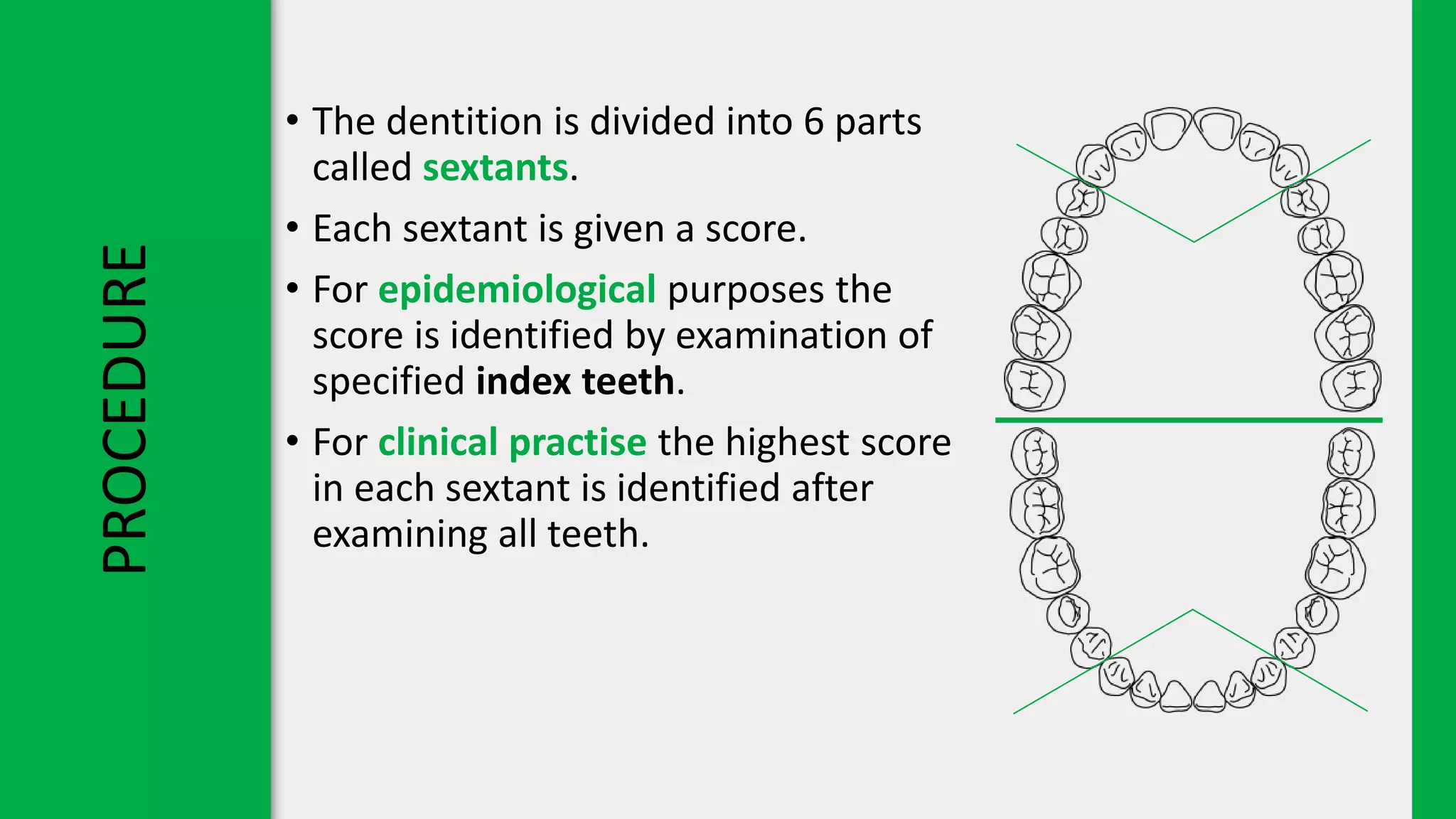

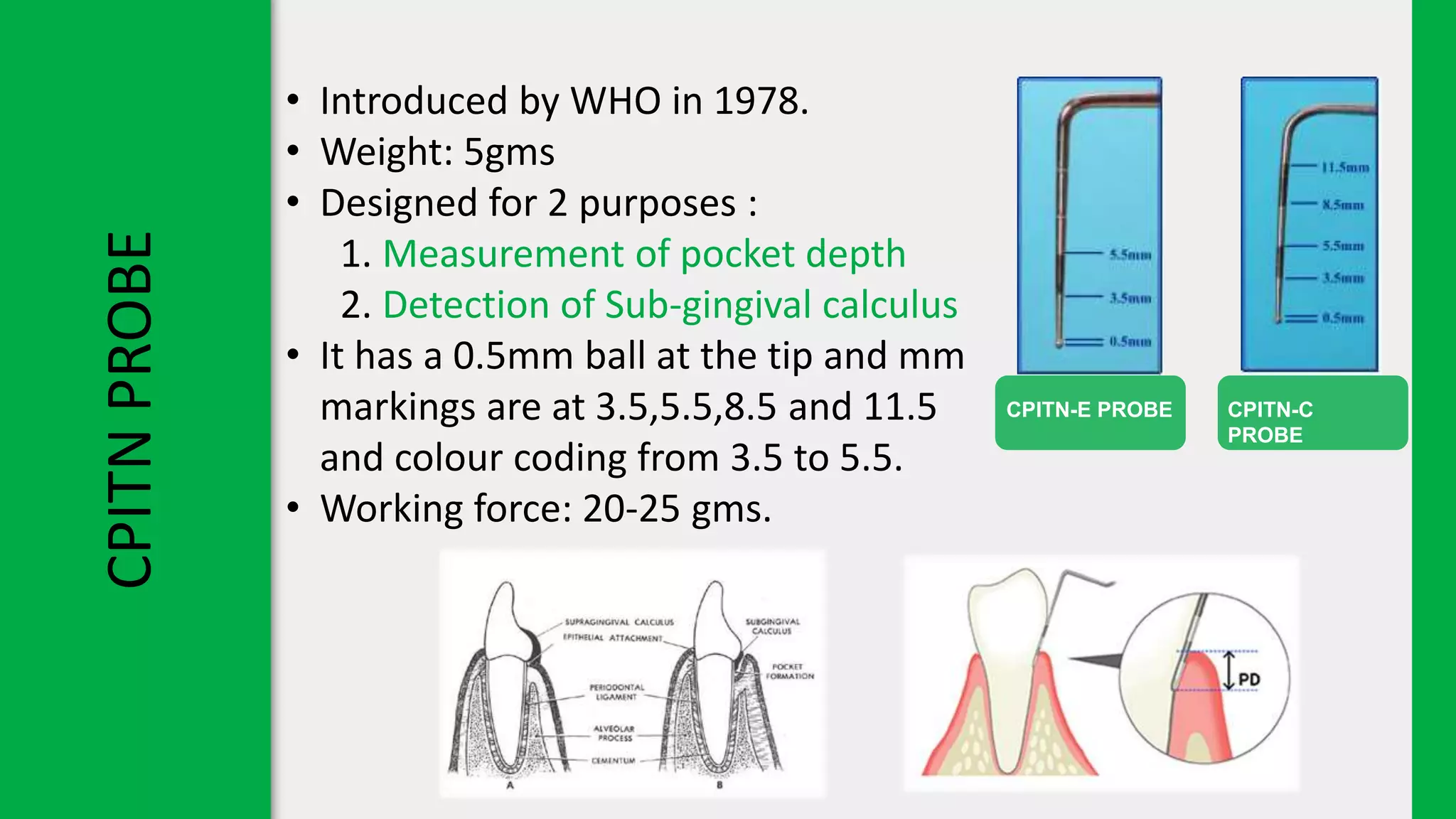
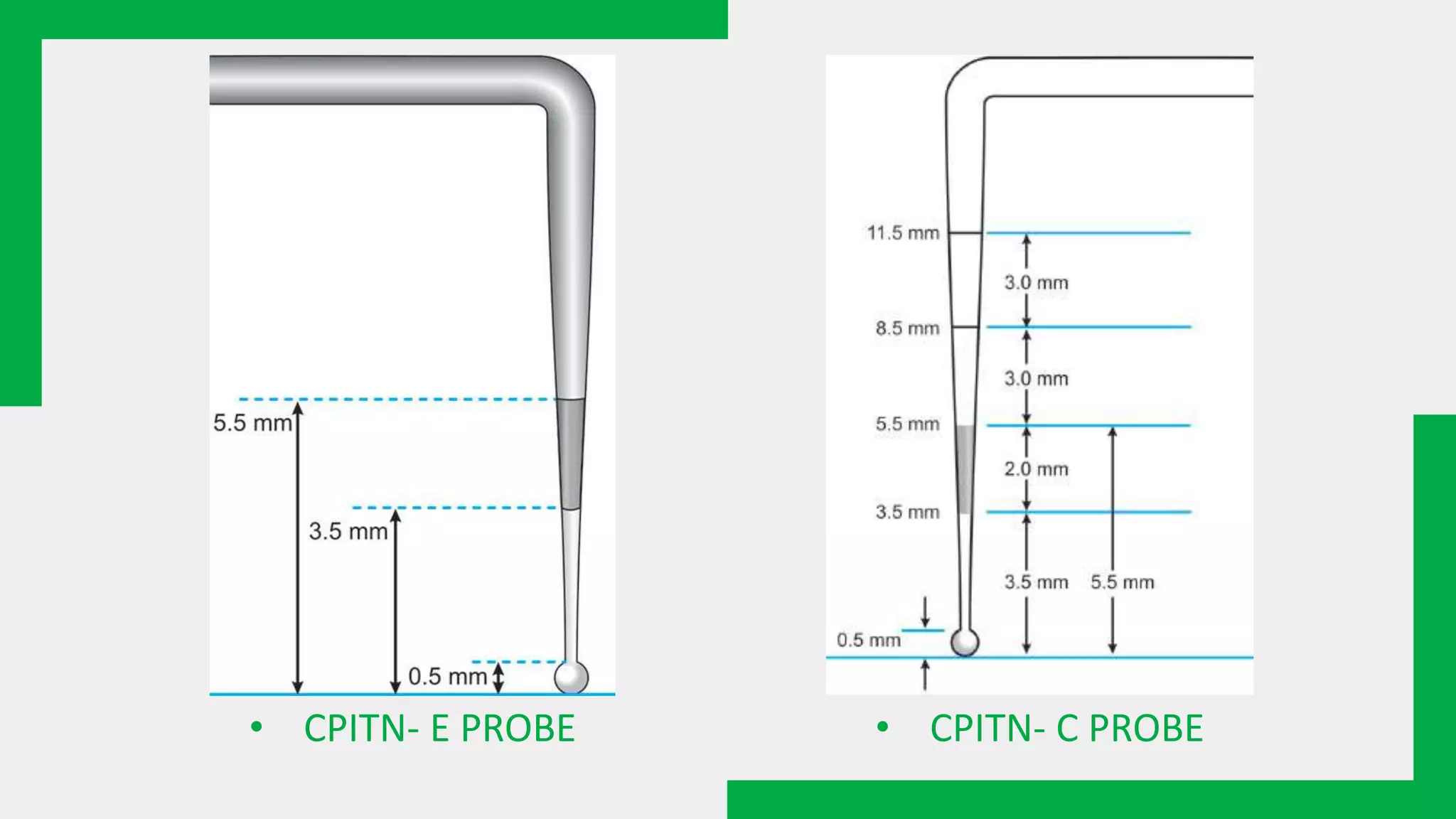
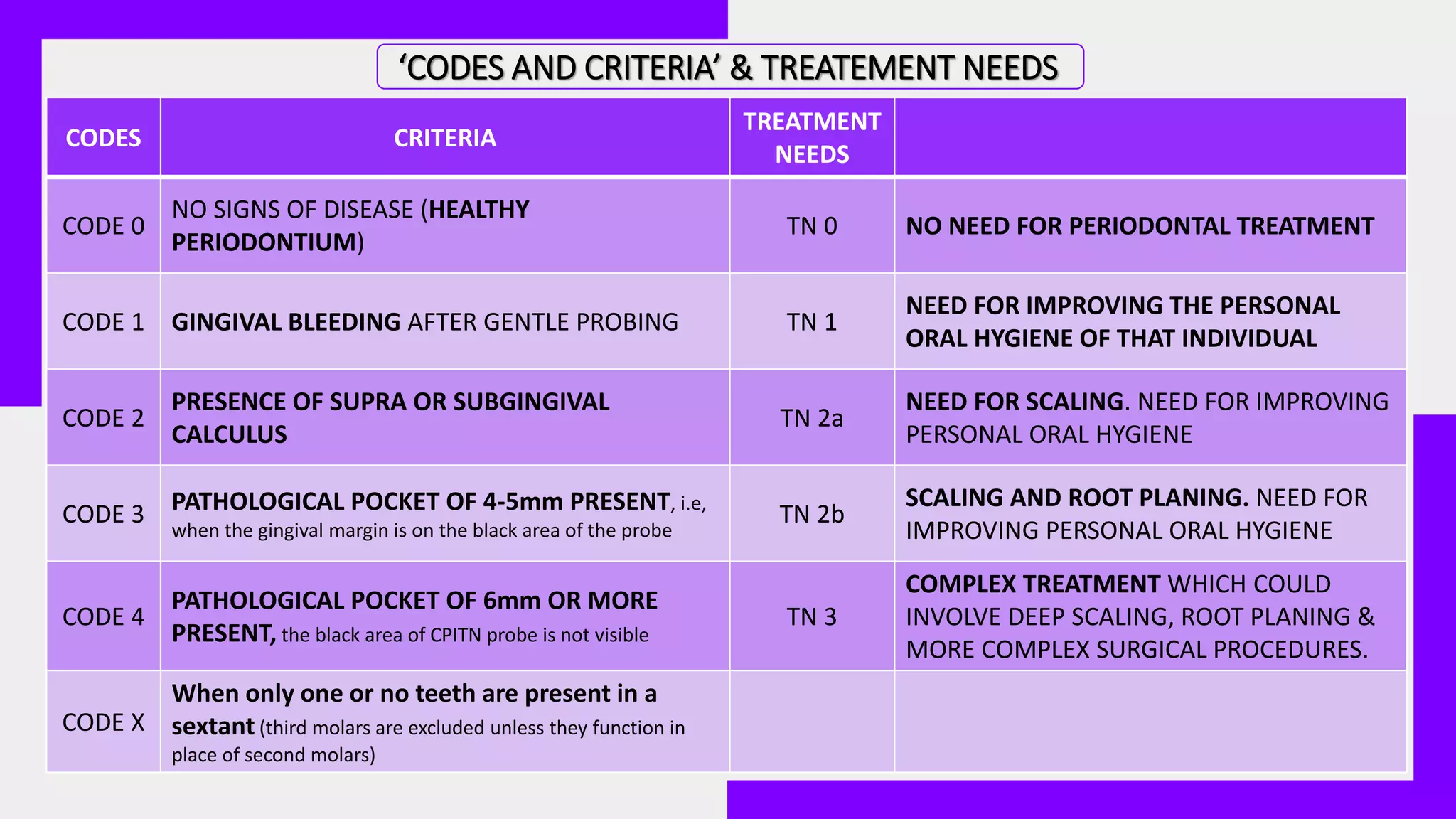
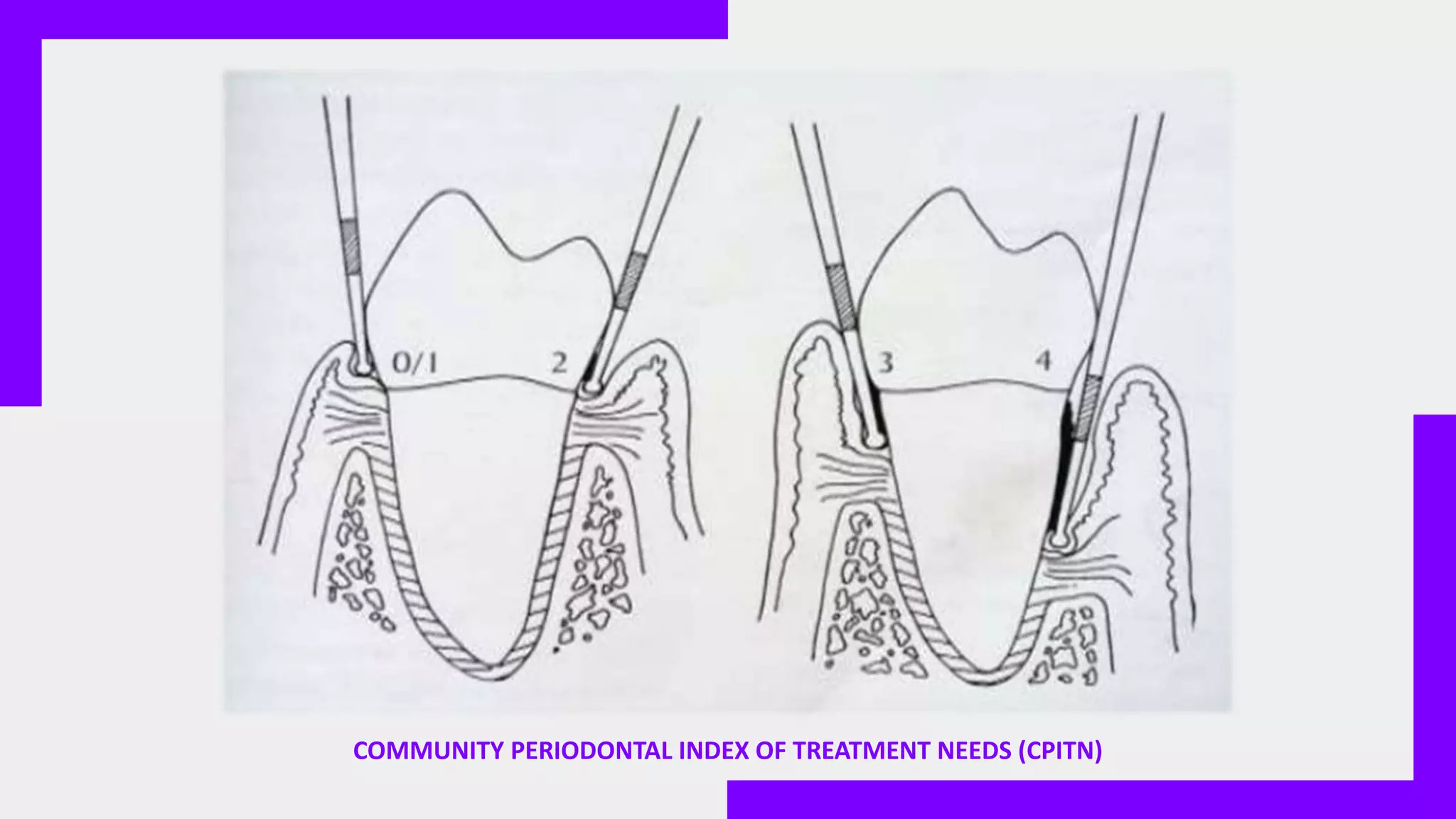


The document presents the Community Periodontal Index of Treatment Needs (CPITN), a dental health assessment tool introduced in 1982 that focuses on evaluating periodontal treatment needs rather than past conditions. It outlines the procedures, instruments and criteria used in its application, which includes probing with a specialized CPITN probe and scoring different periodontal conditions. Additionally, it mentions the Community Periodontal Index (CPI) as a modified version of CPITN that includes loss of attachment measurement.