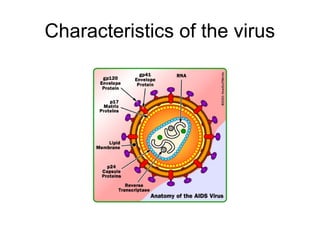
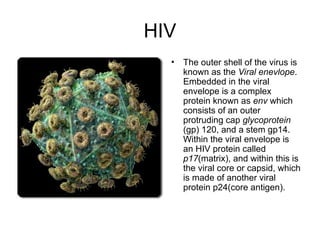
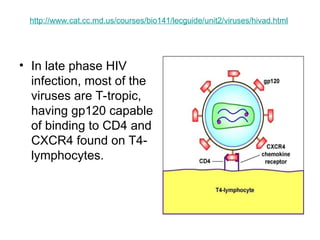
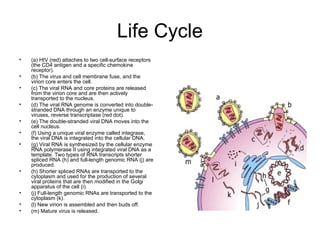
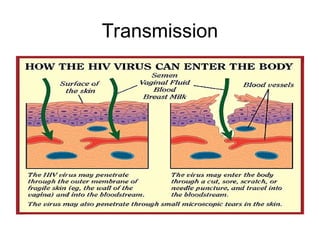
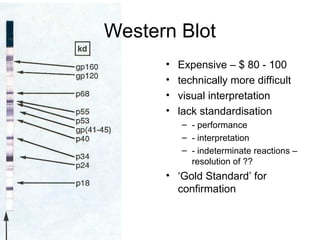
The document provides an overview of the Retroviridae family of viruses, highlighting their significance in diseases like cancer and AIDS, particularly focusing on the human immunodeficiency virus (HIV). It explains the mechanisms of HIV infection, its transmission, and the progression of the disease to AIDS, along with the structure and replication cycle of the virus. Additionally, it discusses the clinical implications, immune responses, and treatment options available for managing HIV infection.



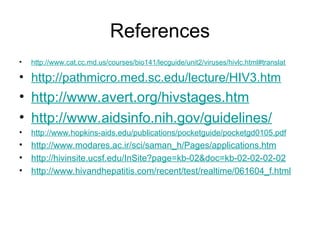
![Hepatitis viruses classification
HAV HBV HCV HDV HEV
Transmission Enteral Parenteral Parenteral Parenteral Enteral
Classification Picornavirus Orthohepadn
avirus
Hepacivirus Deltavirus Hepevirus
Genome +ssRNA dsDNA-RT +ssRNA −ssRNA +ssRNA
Antigens
HBsAg,
HBeAg
Core antigen Delta antigen
Incubation
period
20–40 days 45–160 days 15–150 days 30–60 days 15–60 days
Severity/
Chronicity[5]
Mild; acute
Occasionally
severe; 5–
10% chronic
Subclinical;
70% chronic
Exacerbates
symptoms of
HBV; chronic
with HBV
Mild in normal
patients;
severe in
pregnant
women; acute
Vaccine
10 year
protection
3 injections,
lifetime
protection
None
available
None
available
Investigational
(approved in
China)](https://image.slidesharecdn.com/retroviridae-hiv-250202155201-c629811a/85/Retroviridae-HIV-ppt-presentation-power-68-320.jpg)