• A varietyof human diseases are caused by immune
responses to environmental antigens that lead to
CD4+ TH2 differentiation and production of IgE that
are specific for the antigens and bind to Fc receptors
on mast cells and basophils.
• When they are cross-linked by antigen, the cells are
activated to rapidly release a variety of mediators
which collectively cause increase in vascular
permeability, vasodilation, and bronchial and visceral
smooth muscle contraction.
3.
• Since thesereactions begin rapidly, within minutes
of antigen challenge (immediate), and have major
pathologic consequences (hypersensitivity), they are
referred to as immediate hypersensitivity reactions
• These reactions are called allergy or atopy in clinical
medicine.
• The resulting diseases have a major inflammatory
component triggered by cytokines produced by CD4+
TH2 and mast cells
4.
General Features ofImmediate
Hypersensitivity Reactions
• The hallmarks of allergic diseases are the activation of
CD4+ TH2 cells and the production of IgE antibodies
• The typical sequence of events consists of exposure
to an antigen, activation of CD4+ TH2 and B cells
specific for the antigen, production of IgE, binding of
the antibody to Fc receptors of mast cells
(sensitization), and triggering of the mast cells by re-
exposure to the antigen, resulting in the release of
mediators from the mast cells and subsequent
pathologic reaction
5.
• There isa strong genetic predisposition for the
development of immediate hypersensitivity
• The allergens are usually common environmental proteins
and chemicals
• The cytokines produced by TH2 cells are responsible for
many of the features of immediate hypersensitivity
• The clinical and pathologic manifestations of immediate
hypersensitivity consist of the vascular and smooth muscle
reaction that develops rapidly after repeat exposure to the
allergen and a delayed late-phase reaction consisting mainly
of inflammation
6.
• Immediate hypersensitivityreactions are
manifested in different ways, including skin
and mucosal allergies, food allergies, asthma,
and systemic anaphylaxis.
7.
Production of IgE
•Responsible for sensitizing mast cells and
provides recognition of antigen for immediate
hypersensitivity reactions.
- Atopic individuals produce high levels of IgE in
response to environmental allergens, whereas
normal individuals generally synthesize other
isotypes, such as IgM and IgG, and only small
amounts of IgE
8.
The Nature ofAllergens
• Allergens are proteins or chemicals bound to
proteins to which the atopic individual is
chronically exposed. Examples are proteins in
pollen, house dust mites, animal dander,
foods, and chemicals like the antibiotic
penicillin. Typical features of many common
allergens are low molecular weight,
glycosylation, and high solubility in body fluids
9.
Binding of IgEto Mast Cells and Basophils
• Mast cells and basophils express a high-affinity
Fc receptor specific for ε heavy chains called
FcεRI that binds IgE with a very high affinity (1
x 10^-10).
10.
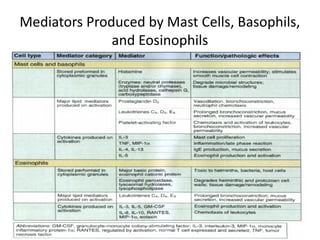
Role of MastCells, Basophils, and
Eosinophils in Immediate Hypersensitivity
• Basophils are blood granulocytes with structural and
functional similarities to mast cells
• Eosinophils are bone marrow-derived granulocytes
that are abundant in the inflammatory infiltrates of
late phase reactions
• All three cell types contain cytoplasmic granules
whose contents are the major mediators of allergic
reactions
• All three produce lipid mediators and cytokines that
induce inflammation
Reactions of ImmediateHypersensitivity
• Divided into immediate and late phase
reactions where IgE and mast cells are the
mediators.
• Immediate reactions are characterized by
vascular and smooth muscle responses to
mediators while late-phase reactions are
mediated by leukocyte recruitment and
inflammation
15.
The Immediate Reaction
•The early vascular changes that occur during immediate
hypersensitivity reactions are demonstrated by the wheal
and flare reaction to the intradermal injection of an
allergen.
- The injection site becomes red and then swells as a result
of leakage of plasma from the venules.
- Blood vessels at the margins of the wheal dilate and
become engorged with RBCs and produce a characteristic
red rim called flare.
- The full reaction can take 5 to 10 minutes and then subside
usually in less than an hour
16.
• The whealand flare reaction results from
sensitization of dermal mast cells by IgE bound
to FcεRI, cross-linking of the IgE by the
antigen, and activation of mast cells and
release of mediators, most notably histamine
17.
The Late-Phase Reaction
•The Immediate wheal and flare reaction is
followed 2 to 4 hours later by a late-phase
reaction consisting of the accumulation of
inflammatory leukocytes, including
neutrophils, eosinophils, basophils, and Th2
cells.
- The inflammation is maximal by about 24 hours
and then gradually subsides.
18.
• The late-phasereaction may occur without a
detactable preceding immediate
hypersensitivity reaction e.g. in asthma. In this
case, there is very little mast cell activation
and the cytokines that sustain the late-phase
reaction may be produced mainly by T cells
19.
Allergic Diseases inHumans: Pathogenesis
and Therapy
• Mast cell degranulation is a central
component of all allergic diseases, and the
clinical and pathologic manifestations of the
diseases depend on the tissues in which the
mast cell mediators have effects as well as the
chronicity of the resulting inflammation
process.
20.
Systemic anaphylaxis
• Characterizedby edema in many tissues and a fall in
blood pressure secondary to vasodilation
• The mainstay of treatment is systemic epinephrine,
which can be lifesaving by reversing the
bronchoconstrictive and vasodilatory effects of the
various mast cell mediators
• Epinephrine also improves cardiac output, further
aiding survival from threatened circulatory collapse.
• Antihistamines may also be beneficial in anaphylaxis,
suggesting a role for histamine in this reaction
21.
Bronchial Asthma
• Inflammatorydisease caused by repeated immediate
hypersensitivity and late-phase reactions in the lung
leading to the clinicopathologic triad of intermittent
and reversible airway obstruction, chronic bronchial
inflammation with eosinophils, and bronchial
smooth muscle cell hypertrophy and hyperreactivity
to bronchoconstrictors
• Current therapy for asthma has two major targets:
prevention and reversal of inflammation and
relaxation of airway smooth muscle
22.
• Corticosteroids blockthe production of
inflammatory cytokines while sodium
chromolyn appears to antagonize IgE-induced
release of mediators. Both agents can be used
prophylactically as inhalants
• Major drugs used are activators of adenylate
cyclase such as epinephrine and related β2-
adrenergic agents
23.
Allergic rhinitis
• Akahay fever. Perhaps the most common
allergic disease
• A consequence of reaction to plant pollen or
house dust mites localized to the upper
respiratory tract by inhalation
• Allergic conjunctivitis with itchy eyes is
commonly associated with rhinitis
• Antihistamines are the most common drugs
24.
Food allergies
• Reactionsto ingested foods that lead to the
release of mediators from intestinal mucosal
and submucosal mast cells.
• Most common allergens are peanuts and
shellfish
25.
Other Immunotherapy strategiesfor Allergic
Diseases
• Desensitization
• Systemic administration of humanized
monoclonal anti-IgE antibodies