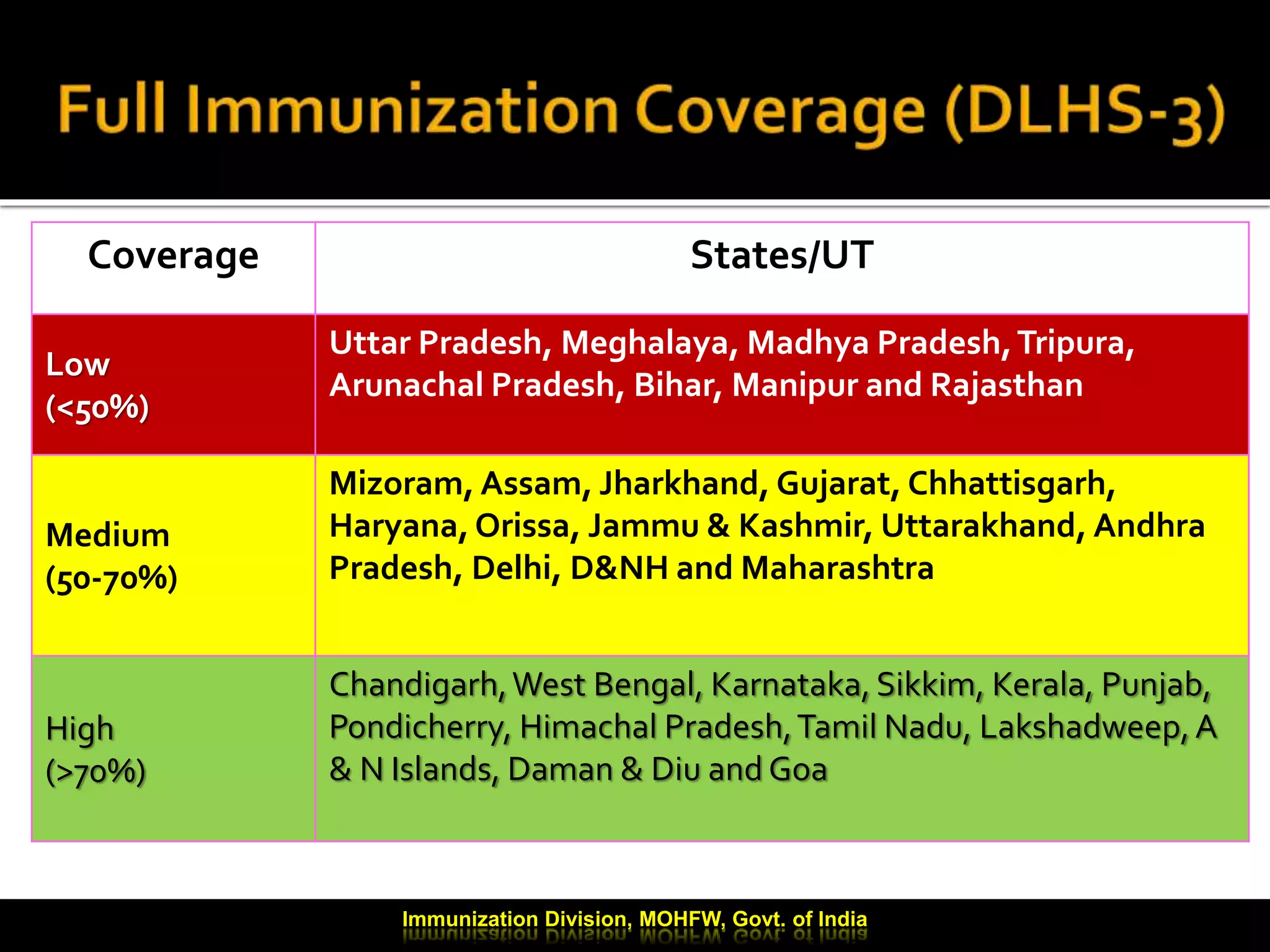
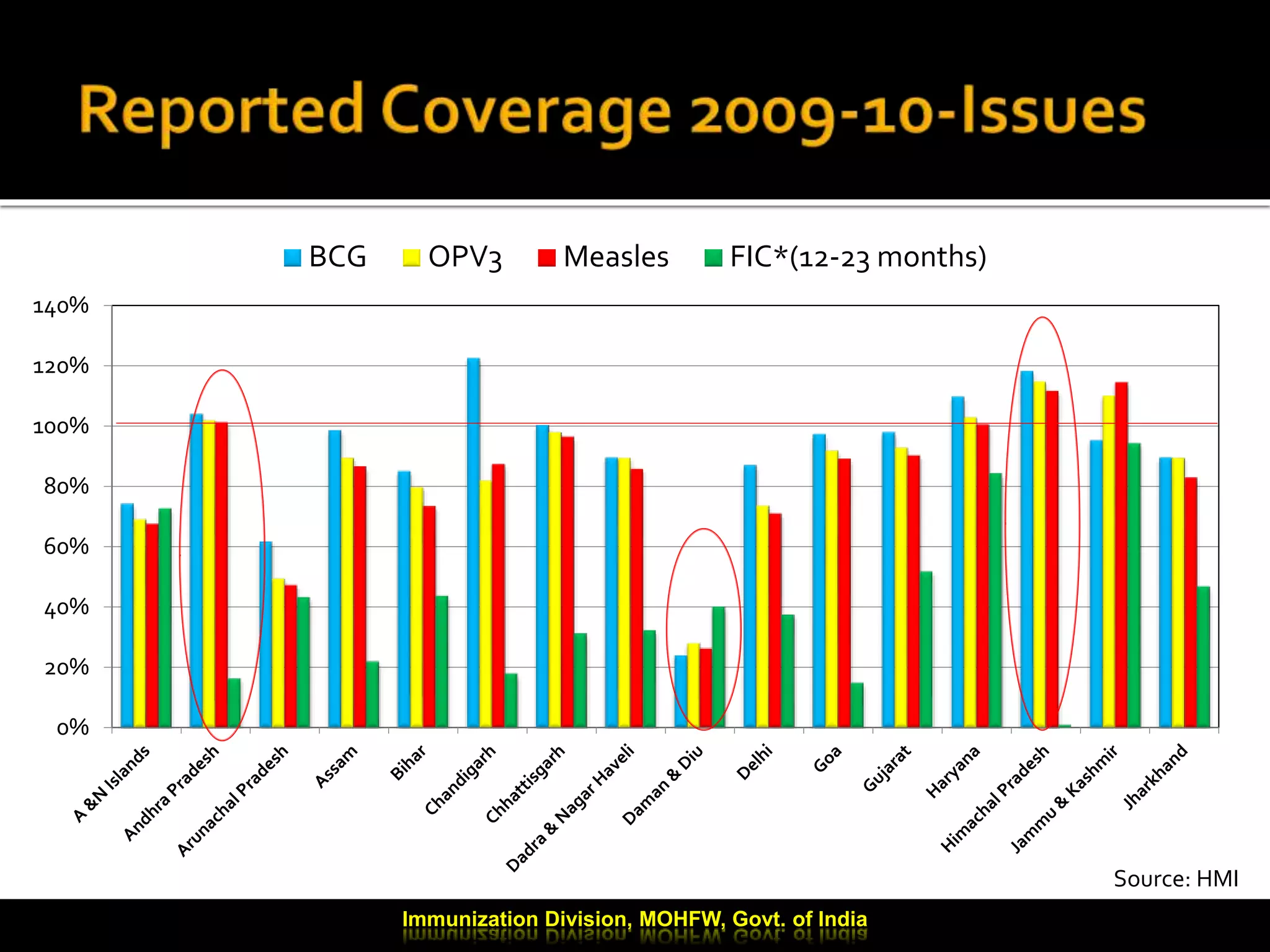
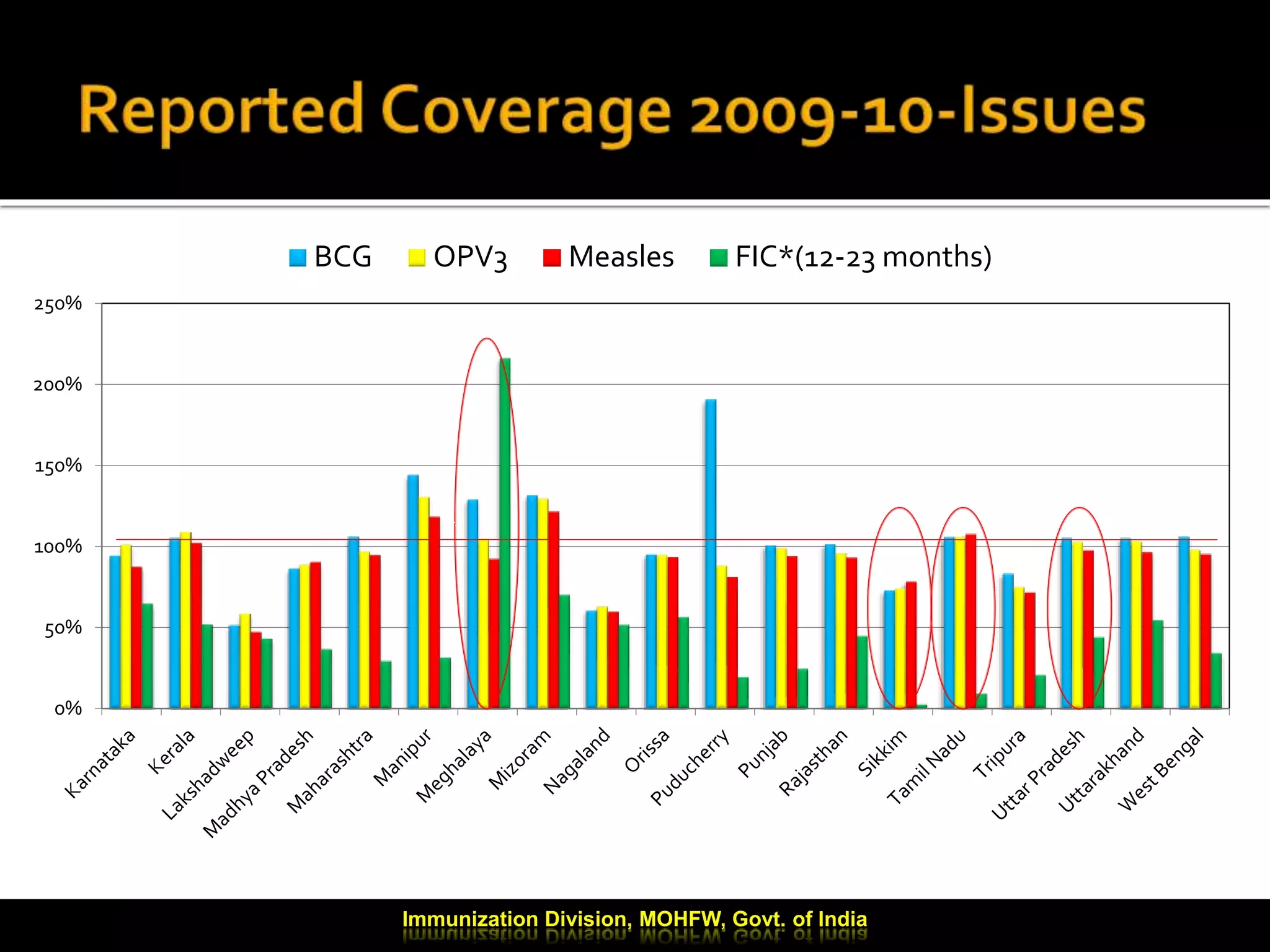
This document provides an update on India's immunization program. It notes that the program is one of the largest public health interventions in the country, targeting over 26 million infants and 30 million pregnant women in 2009-2010. It is centrally sponsored under the National Rural Health Mission. The document reviews coverage levels by state, discusses progress in training health workers, and outlines plans to introduce additional vaccines like hepatitis B and pentavalent vaccines in more states. It also addresses ongoing challenges like improving routine immunization coverage and strengthening cold chain management.