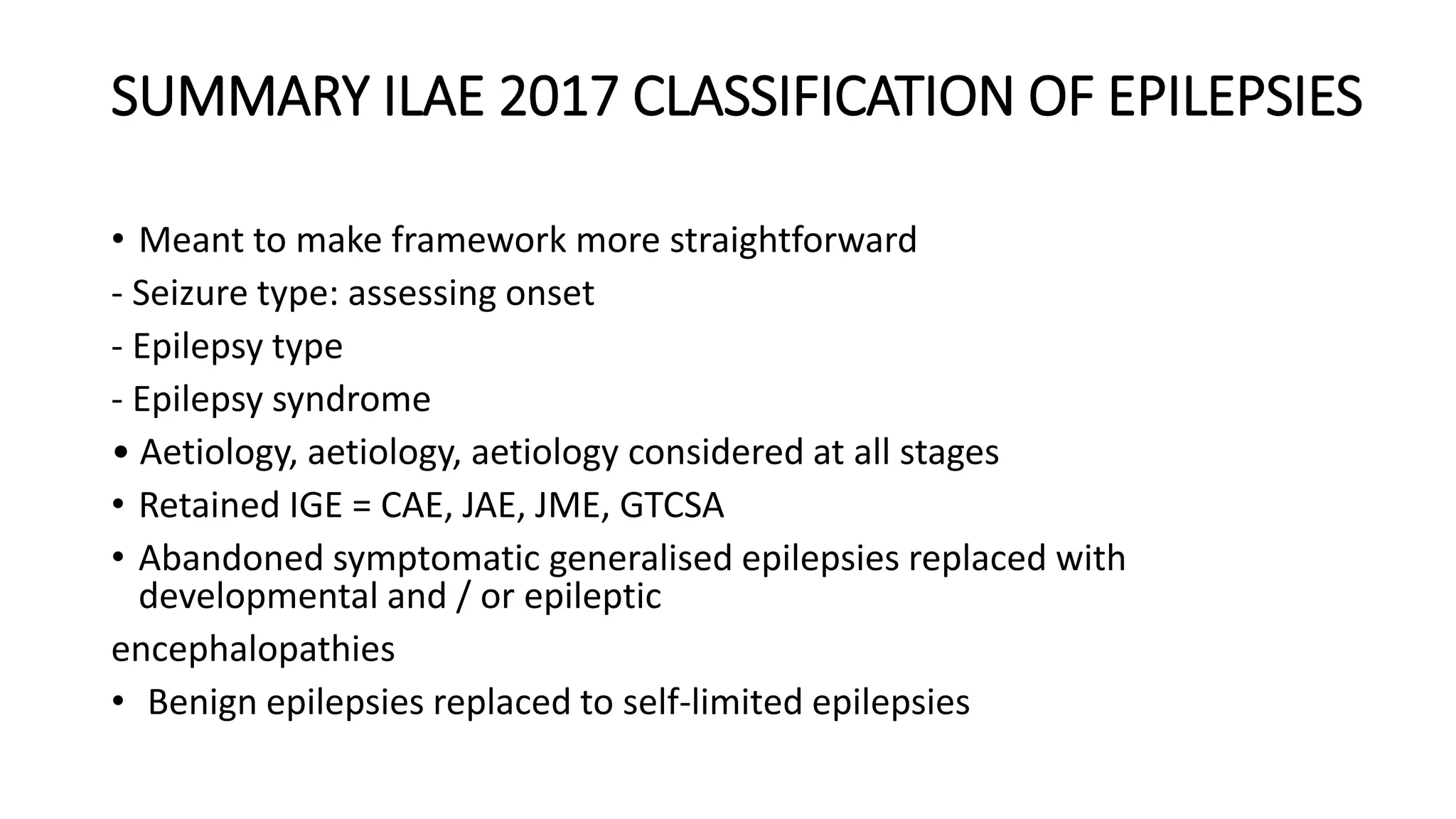
1) The document defines epilepsy and provides the new ILAE 2017 classification framework for epilepsy syndromes.
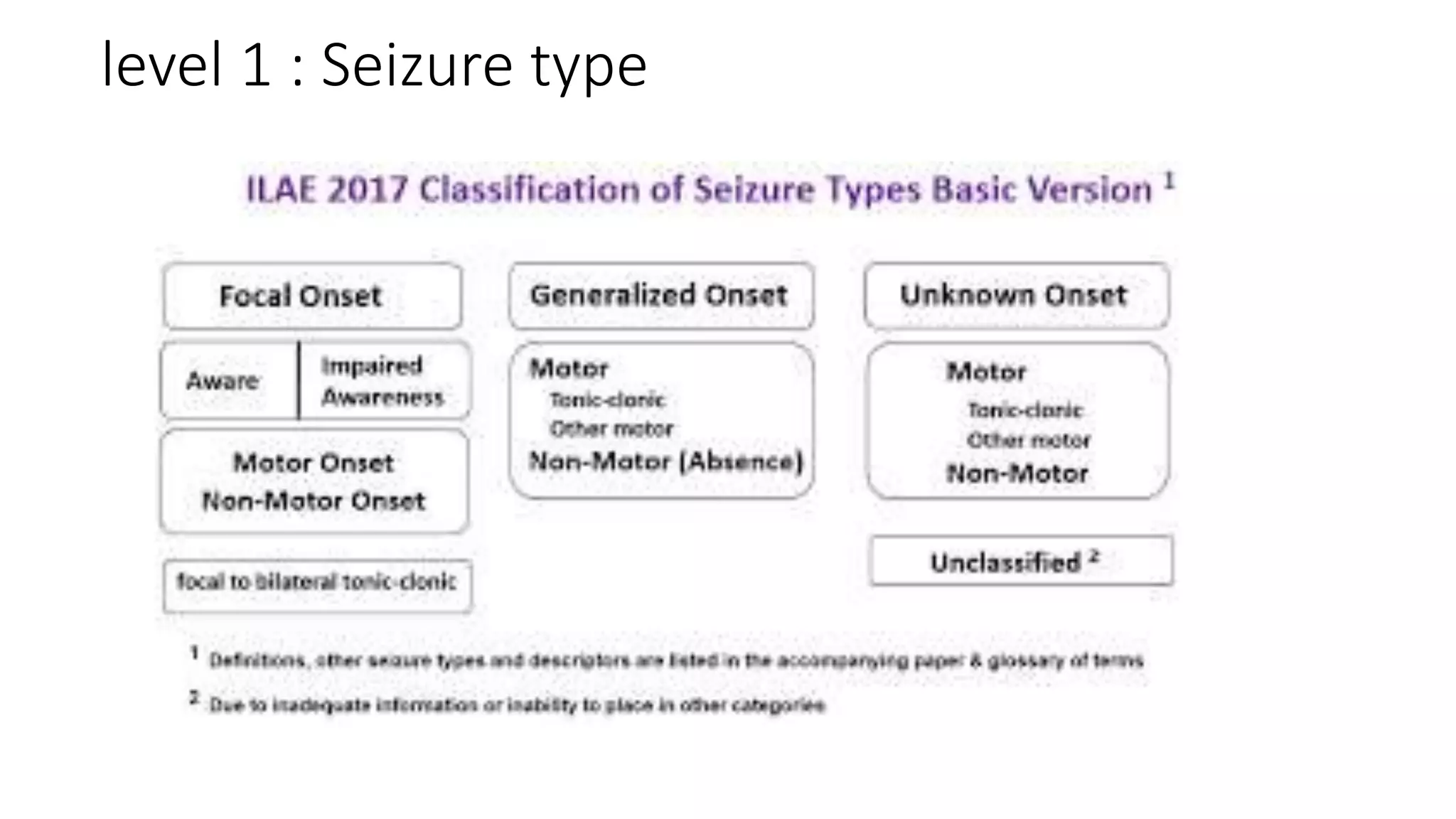
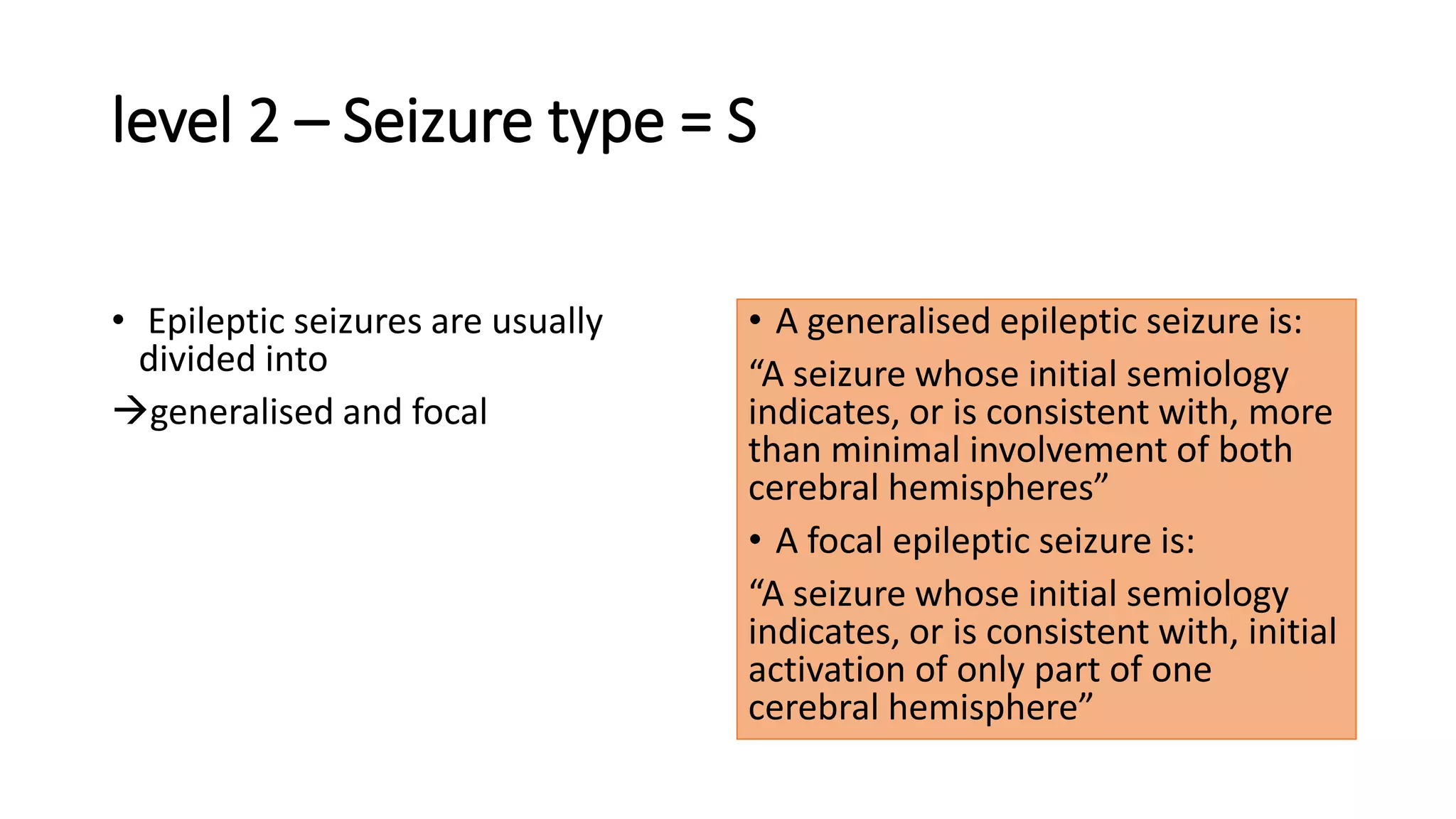
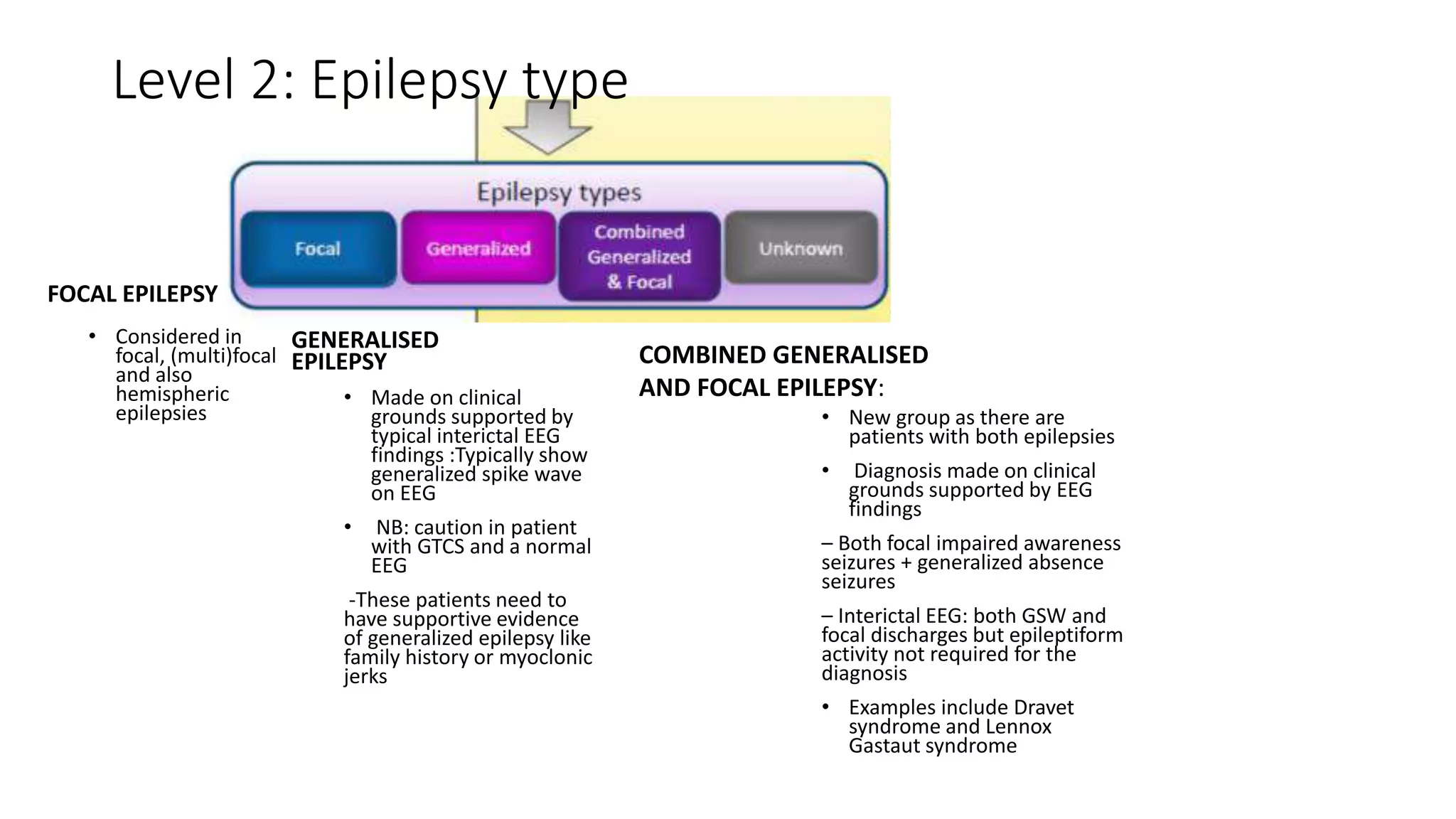
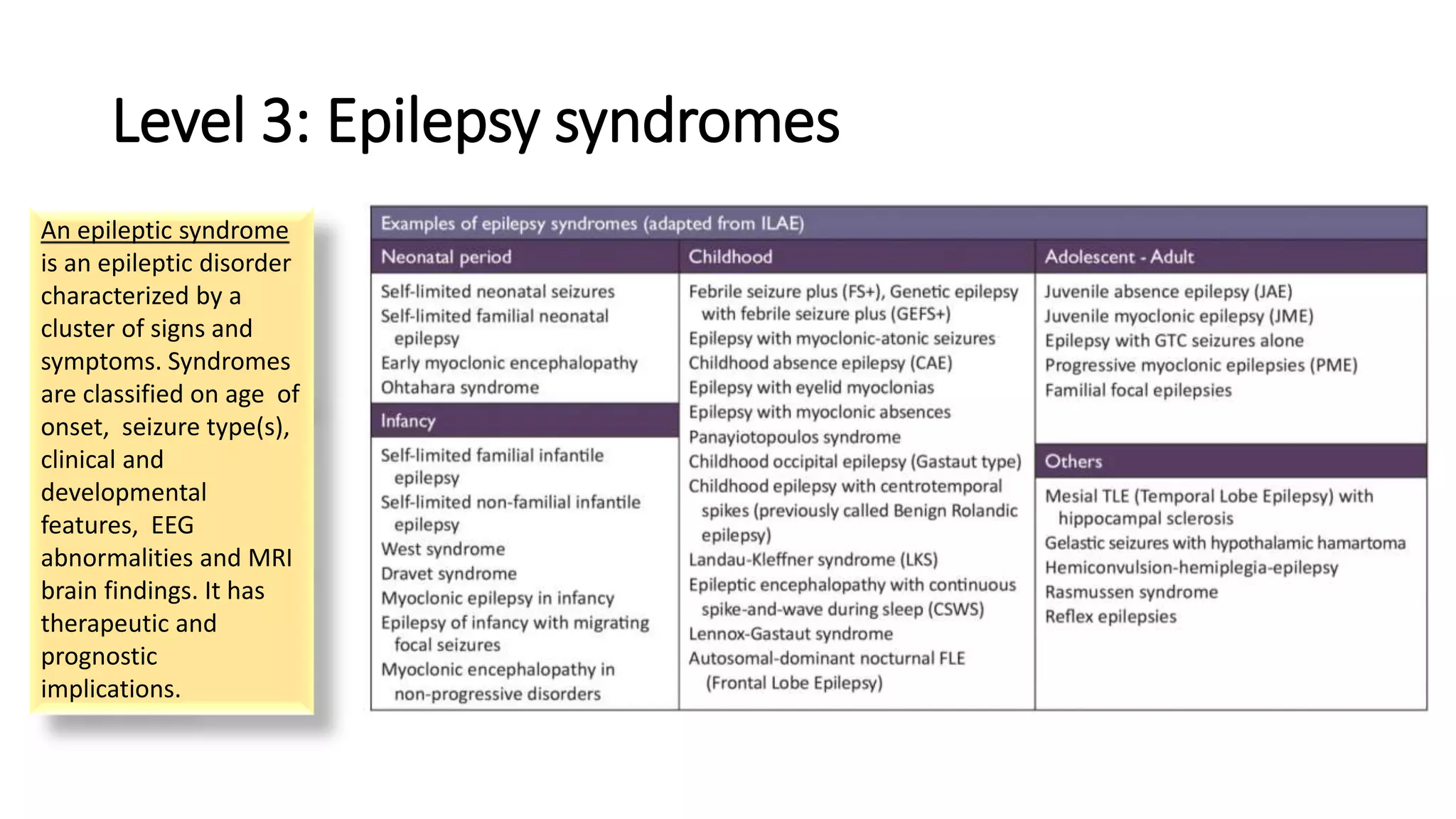
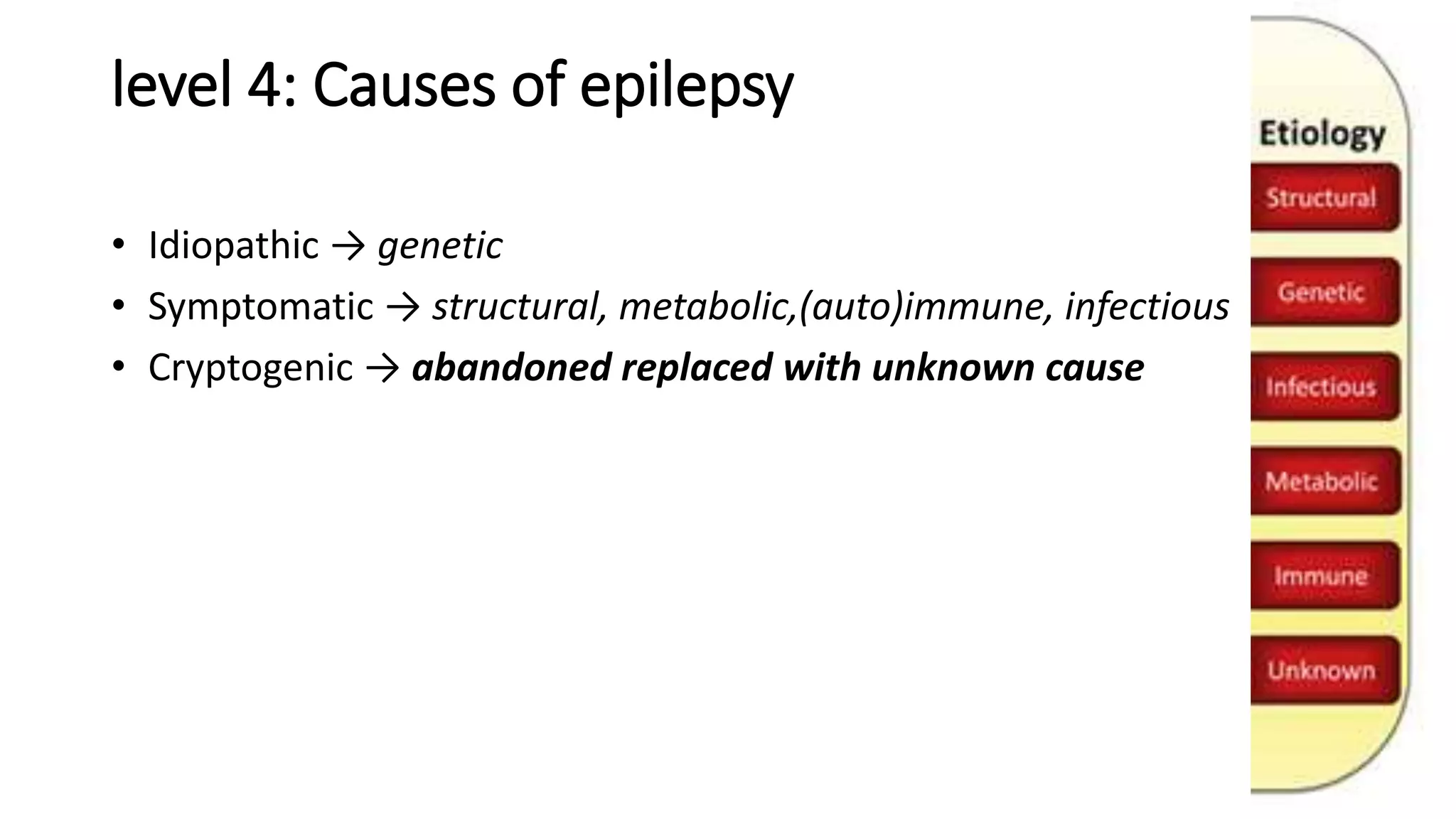
2) The classification involves assessing the seizure type, epilepsy type, syndrome, cause, and other relevant impairments.
3) Classifying epilepsy according to this framework helps to determine appropriate testing, treatment, and prognosis for patients. It provides a standardized method for clinicians.