
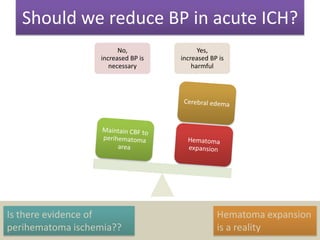
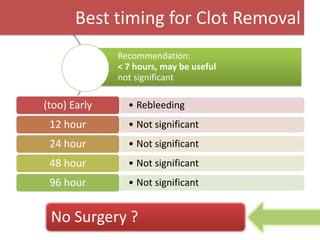
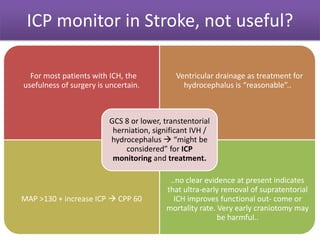


This document summarizes key issues and guidelines for the management of intracerebral hemorrhage (ICH). It discusses debates around blood pressure management, timing of clot removal, use of ICP monitoring, and role of surgery. The guidelines note that while increased blood pressure may be necessary, it could also be harmful. Clot removal within 7 hours may be useful but is not significantly beneficial at later time points. ICP monitoring is not generally useful for most ICH patients but could be considered for those with GCS 8 or lower and signs of herniation or hydrocephalus. The role of surgery is uncertain and early craniotomy may be harmful. In conclusion, guidelines provide admissions that more evidence is still needed





![Intracerebral hemorrhage, SAH, ischemic stroke,[412].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/intracerebralhemorrhagesahischemicstroke412-230303063307-468e029c-thumbnail.jpg?width=640&height=640&fit=bounds)





























































