D.M. was in a motorcycle accident and is confused and disoriented with no memory of the accident. He has a cervical collar and IV fluids started by paramedics as he is transported to the emergency department. Initial vital signs are stable. Scans show signs of brain injury requiring treatment and monitoring to control increased intracranial pressure through interventions like medication, drainage, and careful monitoring of vital signs and neurological status. The long-term prognosis is uncertain but recovery may continue for several months with rehabilitation.
ASSESSMENT AND PLANNING GUIDE FOR USE IN THE HOSPITALThe followi.docxgalerussel59292
ASSESSMENT AND PLANNING GUIDE FOR USE IN THE HOSPITAL
The following information should be included daily as it applies to your patient.
Demographic DataDate of AdmissionVital Signs
39 y/o African American male
10/28/18
BP: 115/60. Pain: 2
P: 91
T: 98.2.
RR: 22
SP02: 95
Significant Past Medical HistoryAllergies/Reactions
HTN, Hyperlipemia, Diabetes
NKA
Reason for Hospitalization and Current Diagnosis
Current Diagnosis: Acute Embolic Stroke, Cerebral Edema, R Hemiparesis, Pneumonia
Reason for hospitalization: 38 y/o male with a history of HTN presented with onset Right Sided Weakness and confusion at 11pm on 10-27-18 when he went to sleep. He woke up at 3am and he was talking gibberish to his fiancé. He went back to sleep and 2 hours later his symptoms had worsened. On 10-28-18, EMS was called by his fiancé and he was taken to the ER. His fiancé said he had taken “something” possibly cocaine. Patient was diagnosed with Acute Embolic Stroke, Cerebral Edema, R Hemiparesis and recently Pnuemonia.
Describe thepathophysiologyincluding signs, symptoms and incidence; and compare with patient findings:
· Acute Embolic Stroke:
Pathophysiology: Occurs when a blood clot that forms somewhere elsewhere in the body breaks loose and then travels to the brain through the bloodstream. The clot can lodge in an artery and blocks the flow of blood.
Common symptoms:Difficulty speaking or understanding words, numbness and tingling, temporary paralysis, blurred vision or blindness, slurred speech, dizziness, feeling faint, difficulty swallowing, nausea, sleepiness. Embolic stroke doesn’t cause any unique symptoms
Muscular symptoms: Difficulty with coordination, stiff muscles, feelings of weakness on one side or all of the body.
Cognitive symptoms: Mental confusion, an altered level of consciousness, visual agnosia
Patient Findings: Patient presented with R hemiparesis, facial drooping, slurred speech, difficulty swallowing.
· Cerebral Edema
Pathophysiology: It’s a life threatening condition that causes fluid to develop in the brain.
This fluid increases the pressure inside of the skull causing intracranial pressure (ICP). Increased ICP can reduce brain blood flow and decrease the oxygen your brain receives. The brain needs an uninterrupted flow of oxygen to function properly.
Symptoms: Headache, dizziness, nausea, lack of coordination, numbness, mood changes, memory loss, difficulty speaking, incontinence, change in consciousness, seizures, weakness in extremities
Patient Findings: Patient presented with difficulty speaking, incontinence, change in consciousness, weakness in extremities
· Hemiparesis
Pathophysiology: Hemiparesis is weakness on one side of the body. One side can still move but with reduced muscular strength.
Symptoms: Difficulty walking, standing, and maintaining your balance. You may also have numbness or tingling on your weaker side.
Patient findings: Patient has right sided weakness.
· Pneumonia
.
ASSESSMENT AND PLANNING GUIDE FOR USE IN THE HOSPITALThe followi.docxgalerussel59292
ASSESSMENT AND PLANNING GUIDE FOR USE IN THE HOSPITAL
The following information should be included daily as it applies to your patient.
Demographic DataDate of AdmissionVital Signs
39 y/o African American male
10/28/18
BP: 115/60. Pain: 2
P: 91
T: 98.2.
RR: 22
SP02: 95
Significant Past Medical HistoryAllergies/Reactions
HTN, Hyperlipemia, Diabetes
NKA
Reason for Hospitalization and Current Diagnosis
Current Diagnosis: Acute Embolic Stroke, Cerebral Edema, R Hemiparesis, Pneumonia
Reason for hospitalization: 38 y/o male with a history of HTN presented with onset Right Sided Weakness and confusion at 11pm on 10-27-18 when he went to sleep. He woke up at 3am and he was talking gibberish to his fiancé. He went back to sleep and 2 hours later his symptoms had worsened. On 10-28-18, EMS was called by his fiancé and he was taken to the ER. His fiancé said he had taken “something” possibly cocaine. Patient was diagnosed with Acute Embolic Stroke, Cerebral Edema, R Hemiparesis and recently Pnuemonia.
Describe thepathophysiologyincluding signs, symptoms and incidence; and compare with patient findings:
· Acute Embolic Stroke:
Pathophysiology: Occurs when a blood clot that forms somewhere elsewhere in the body breaks loose and then travels to the brain through the bloodstream. The clot can lodge in an artery and blocks the flow of blood.
Common symptoms:Difficulty speaking or understanding words, numbness and tingling, temporary paralysis, blurred vision or blindness, slurred speech, dizziness, feeling faint, difficulty swallowing, nausea, sleepiness. Embolic stroke doesn’t cause any unique symptoms
Muscular symptoms: Difficulty with coordination, stiff muscles, feelings of weakness on one side or all of the body.
Cognitive symptoms: Mental confusion, an altered level of consciousness, visual agnosia
Patient Findings: Patient presented with R hemiparesis, facial drooping, slurred speech, difficulty swallowing.
· Cerebral Edema
Pathophysiology: It’s a life threatening condition that causes fluid to develop in the brain.
This fluid increases the pressure inside of the skull causing intracranial pressure (ICP). Increased ICP can reduce brain blood flow and decrease the oxygen your brain receives. The brain needs an uninterrupted flow of oxygen to function properly.
Symptoms: Headache, dizziness, nausea, lack of coordination, numbness, mood changes, memory loss, difficulty speaking, incontinence, change in consciousness, seizures, weakness in extremities
Patient Findings: Patient presented with difficulty speaking, incontinence, change in consciousness, weakness in extremities
· Hemiparesis
Pathophysiology: Hemiparesis is weakness on one side of the body. One side can still move but with reduced muscular strength.
Symptoms: Difficulty walking, standing, and maintaining your balance. You may also have numbness or tingling on your weaker side.
Patient findings: Patient has right sided weakness.
· Pneumonia
.
1
15
Academic Clinical History & Physical Notes for Cerebral Ischemia
Muhammad Aftkhar
Grand Canyon University
December 04th, 2020
Academic Clinical History & Physical Notes for Cerebral Ischemia
I am presenting the academic clinical history and physical notes for the patient of ischemic stroke. Ischemic stroke or cerebral ischemia occurs when one of the cerebral arteries is blocked by the clot leading to diminished blood supply and oxygen to brain cells resulting in damage or death of brain cells (Celik et al., 2020)
History and Physical Note
1.Chief complaint/reason for admission/visit/consult.
A 52 years old male patient came to the acute care hospital with the chief complaint of sudden severe headache, dizziness, and slurred speech.
HPI for the H&P or consult notes.
The patient felt a severe burning and shooting pain in the frontal region of the head while he was reading the newspaper in the morning. The patient said that he developed blurred vision during reading. The patient felt numbness when the pain started (Harriot et al., 2020). The patient said that the pain was not subsiding with the time as it persisted since its onset. The pain scale was nine by 10, started in the frontal region, and radiated towards the temporal region. The associated symptoms with pain are nausea, vomiting, aphasia, dysarthria, apraxia, and vertigo (De Cock, et al., 2020). The symptoms become aggravate in a standing position and become alleviating when he lay down on the bed with 3 pillows. The patient felt a significant change in body posture. He is positive for facial drooping while negative for fever and chills. He finds difficulty in sitting and maintaining coordination. The patient stated that he had a medical history of neck trauma in a road accident. He was hospitalized for 3 weeks after neck surgery.
2.Medical, surgical, family, social, and allergy history.
Medical history
The patient has hypertension and hypercholesterolemia (Haegens, et al., 2018).
Surgical history
The patient underwent neck surgery after neck trauma at the age of 42.
Family history
The patient’s mother is alive and diabetic. The father of the patient died due to a cardiac stroke. His sister is normal. One of the two brothers has hypertension, and the other is normal. Currently, the patient is living with his normal wife.
Social history
The patient has a long history of smoking and boozing, coupled with a sedentary lifestyle.
Allergy history
· Raw fruits and vegetables, Shellfish, Soy.
· Amoxicillin and aspirin.
3.Home medications, including dosages, route, frequency, and current medications, if a consultation note.
Antihypertensive drugs Edarbi & Hygroton.
40 mg oral Edarbi once a day, as the patient is on diuretics, Hygroton. Oral 50 mg Hygroton once in the morning.
Hypercholesterolemic drugs Lipitor
Oral tablet 40 mg once a day. He takes this tablet at night.
4.Review of systems with all body systems for H&P or consult notes. Review of systems i ...
1
15
Academic Clinical History & Physical Notes for Cerebral Ischemia
Muhammad Aftkhar
Grand Canyon University
December 04th, 2020
Academic Clinical History & Physical Notes for Cerebral Ischemia
I am presenting the academic clinical history and physical notes for the patient of ischemic stroke. Ischemic stroke or cerebral ischemia occurs when one of the cerebral arteries is blocked by the clot leading to diminished blood supply and oxygen to brain cells resulting in damage or death of brain cells (Celik et al., 2020)
History and Physical Note
1.Chief complaint/reason for admission/visit/consult.
A 52 years old male patient came to the acute care hospital with the chief complaint of sudden severe headache, dizziness, and slurred speech.
HPI for the H&P or consult notes.
The patient felt a severe burning and shooting pain in the frontal region of the head while he was reading the newspaper in the morning. The patient said that he developed blurred vision during reading. The patient felt numbness when the pain started (Harriot et al., 2020). The patient said that the pain was not subsiding with the time as it persisted since its onset. The pain scale was nine by 10, started in the frontal region, and radiated towards the temporal region. The associated symptoms with pain are nausea, vomiting, aphasia, dysarthria, apraxia, and vertigo (De Cock, et al., 2020). The symptoms become aggravate in a standing position and become alleviating when he lay down on the bed with 3 pillows. The patient felt a significant change in body posture. He is positive for facial drooping while negative for fever and chills. He finds difficulty in sitting and maintaining coordination. The patient stated that he had a medical history of neck trauma in a road accident. He was hospitalized for 3 weeks after neck surgery.
2.Medical, surgical, family, social, and allergy history.
Medical history
The patient has hypertension and hypercholesterolemia (Haegens, et al., 2018).
Surgical history
The patient underwent neck surgery after neck trauma at the age of 42.
Family history
The patient’s mother is alive and diabetic. The father of the patient died due to a cardiac stroke. His sister is normal. One of the two brothers has hypertension, and the other is normal. Currently, the patient is living with his normal wife.
Social history
The patient has a long history of smoking and boozing, coupled with a sedentary lifestyle.
Allergy history
· Raw fruits and vegetables, Shellfish, Soy.
· Amoxicillin and aspirin.
3.Home medications, including dosages, route, frequency, and current medications, if a consultation note.
Antihypertensive drugs Edarbi & Hygroton.
40 mg oral Edarbi once a day, as the patient is on diuretics, Hygroton. Oral 50 mg Hygroton once in the morning.
Hypercholesterolemic drugs Lipitor
Oral tablet 40 mg once a day. He takes this tablet at night.
4.Review of systems with all body systems for H&P or consult notes. Review of systems i ...
1
15
Academic Clinical History & Physical Notes for Cerebral Ischemia
I am presenting the academic clinical history and physical notes for the patient of ischemic stroke. Ischemic stroke or cerebral ischemia occurs when one of the cerebral arteries is blocked by the clot leading to diminished blood supply and oxygen to brain cells resulting in damage or death of brain cells (Celik et al., 2020)
History and Physical Note
1.Chief complaint/reason for admission/visit/consult.
A 52 years old male patient came to the acute care hospital with the chief complaint of sudden severe headache, dizziness, and slurred speech.
HPI for the H&P or consult notes.
The patient felt a severe burning and shooting pain in the frontal region of the head while he was reading the newspaper in the morning. The patient said that he developed blurred vision during reading. The patient felt numbness when the pain started (Harriot et al., 2020). The patient said that the pain was not subsiding with the time as it persisted since its onset. The pain scale was nine by 10, started in the frontal region, and radiated towards the temporal region. The associated symptoms with pain are nausea, vomiting, aphasia, dysarthria, apraxia, and vertigo (De Cock, et al., 2020). The symptoms become aggravate in a standing position and become alleviating when he lay down on the bed with 3 pillows. The patient felt a significant change in body posture. He is positive for facial drooping while negative for fever and chills. He finds difficulty in sitting and maintaining coordination. The patient stated that he had a medical history of neck trauma in a road accident. He was hospitalized for 3 weeks after neck surgery.
2.Medical, surgical, family, social, and allergy history.
Medical history
The patient has hypertension and hypercholesterolemia (Haegens, et al., 2018).
Surgical history
The patient underwent neck surgery after neck trauma at the age of 42.
Family history
The patient’s mother is alive and diabetic. The father of the patient died due to a cardiac stroke. His sister is normal. One of the two brothers has hypertension, and the other is normal. Currently, the patient is living with his normal wife.
Social history
The patient has a long history of smoking and boozing, coupled with a sedentary lifestyle.
Allergy history
· Raw fruits and vegetables, Shellfish, Soy.
· Amoxicillin and aspirin.
3.Home medications, including dosages, route, frequency, and current medications, if a consultation note.
Antihypertensive drugs Edarbi & Hygroton.
40 mg oral Edarbi once a day, as the patient is on diuretics, Hygroton. Oral 50 mg Hygroton once in the morning.
Hypercholesterolemic drugs Lipitor
Oral tablet 40 mg once a day. He takes this tablet at night.
4.Review of systems with all body systems for H&P or consult notes. Review of systems is what the patient or family/friends tell you (by body system).
General appearance
The patient shows facial we ...
1
15
Academic Clinical History & Physical Notes for Cerebral Ischemia
I am presenting the academic clinical history and physical notes for the patient of ischemic stroke. Ischemic stroke or cerebral ischemia occurs when one of the cerebral arteries is blocked by the clot leading to diminished blood supply and oxygen to brain cells resulting in damage or death of brain cells (Celik et al., 2020)
History and Physical Note
1.Chief complaint/reason for admission/visit/consult.
A 52 years old male patient came to the acute care hospital with the chief complaint of sudden severe headache, dizziness, and slurred speech.
HPI for the H&P or consult notes.
The patient felt a severe burning and shooting pain in the frontal region of the head while he was reading the newspaper in the morning. The patient said that he developed blurred vision during reading. The patient felt numbness when the pain started (Harriot et al., 2020). The patient said that the pain was not subsiding with the time as it persisted since its onset. The pain scale was nine by 10, started in the frontal region, and radiated towards the temporal region. The associated symptoms with pain are nausea, vomiting, aphasia, dysarthria, apraxia, and vertigo (De Cock, et al., 2020). The symptoms become aggravate in a standing position and become alleviating when he lay down on the bed with 3 pillows. The patient felt a significant change in body posture. He is positive for facial drooping while negative for fever and chills. He finds difficulty in sitting and maintaining coordination. The patient stated that he had a medical history of neck trauma in a road accident. He was hospitalized for 3 weeks after neck surgery.
2.Medical, surgical, family, social, and allergy history.
Medical history
The patient has hypertension and hypercholesterolemia (Haegens, et al., 2018).
Surgical history
The patient underwent neck surgery after neck trauma at the age of 42.
Family history
The patient’s mother is alive and diabetic. The father of the patient died due to a cardiac stroke. His sister is normal. One of the two brothers has hypertension, and the other is normal. Currently, the patient is living with his normal wife.
Social history
The patient has a long history of smoking and boozing, coupled with a sedentary lifestyle.
Allergy history
· Raw fruits and vegetables, Shellfish, Soy.
· Amoxicillin and aspirin.
3.Home medications, including dosages, route, frequency, and current medications, if a consultation note.
Antihypertensive drugs Edarbi & Hygroton.
40 mg oral Edarbi once a day, as the patient is on diuretics, Hygroton. Oral 50 mg Hygroton once in the morning.
Hypercholesterolemic drugs Lipitor
Oral tablet 40 mg once a day. He takes this tablet at night.
4.Review of systems with all body systems for H&P or consult notes. Review of systems is what the patient or family/friends tell you (by body system).
General appearance
The patient shows facial we ...
This is a review of a case of an infant admitted to pediatric ICU as a case of epidural hematoma after traumatic brain injury. A brief summary of the most important aspects. Part of the residency teaching program for pediatric residents at the pediatric and neonatology department at Istishari Arab Hospital, Ramallah, Palestine.
1. Initial assessment and management of the trauma patient.pptxWalterBenites2
La primera etapa del curso ATLS (Advanced Trauma Life Support) se conoce como "Evaluación Inicial". En esta etapa, los estudiantes de medicina aprenden un enfoque sistemático y estructurado para evaluar a un paciente traumatizado de manera rápida y eficaz.
La Evaluación Inicial se centra en identificar y abordar de inmediato las lesiones que amenazan la vida del paciente.
Antibiotic Stewardship by Anushri Srivastava.pptxAnushriSrivastav
Stewardship is the act of taking good care of something.
Antimicrobial stewardship is a coordinated program that promotes the appropriate use of antimicrobials (including antibiotics), improves patient outcomes, reduces microbial resistance, and decreases the spread of infections caused by multidrug-resistant organisms.
WHO launched the Global Antimicrobial Resistance and Use Surveillance System (GLASS) in 2015 to fill knowledge gaps and inform strategies at all levels.
ACCORDING TO apic.org,
Antimicrobial stewardship is a coordinated program that promotes the appropriate use of antimicrobials (including antibiotics), improves patient outcomes, reduces microbial resistance, and decreases the spread of infections caused by multidrug-resistant organisms.
ACCORDING TO pewtrusts.org,
Antibiotic stewardship refers to efforts in doctors’ offices, hospitals, long term care facilities, and other health care settings to ensure that antibiotics are used only when necessary and appropriate
According to WHO,
Antimicrobial stewardship is a systematic approach to educate and support health care professionals to follow evidence-based guidelines for prescribing and administering antimicrobials
In 1996, John McGowan and Dale Gerding first applied the term antimicrobial stewardship, where they suggested a causal association between antimicrobial agent use and resistance. They also focused on the urgency of large-scale controlled trials of antimicrobial-use regulation employing sophisticated epidemiologic methods, molecular typing, and precise resistance mechanism analysis.
Antimicrobial Stewardship(AMS) refers to the optimal selection, dosing, and duration of antimicrobial treatment resulting in the best clinical outcome with minimal side effects to the patients and minimal impact on subsequent resistance.
According to the 2019 report, in the US, more than 2.8 million antibiotic-resistant infections occur each year, and more than 35000 people die. In addition to this, it also mentioned that 223,900 cases of Clostridoides difficile occurred in 2017, of which 12800 people died. The report did not include viruses or parasites
VISION
Being proactive
Supporting optimal animal and human health
Exploring ways to reduce overall use of antimicrobials
Using the drugs that prevent and treat disease by killing microscopic organisms in a responsible way
GOAL
to prevent the generation and spread of antimicrobial resistance (AMR). Doing so will preserve the effectiveness of these drugs in animals and humans for years to come.
being to preserve human and animal health and the effectiveness of antimicrobial medications.
to implement a multidisciplinary approach in assembling a stewardship team to include an infectious disease physician, a clinical pharmacist with infectious diseases training, infection preventionist, and a close collaboration with the staff in the clinical microbiology laboratory
to prevent antimicrobial overuse, misuse and abuse.
to minimize the developme
Telehealth Psychology Building Trust with Clients.pptxThe Harvest Clinic
Telehealth psychology is a digital approach that offers psychological services and mental health care to clients remotely, using technologies like video conferencing, phone calls, text messaging, and mobile apps for communication.
More Related Content
Similar to 2023_Sp_Neuro Case Study_Acute Intracranial Problems-1.pptx
1
15
Academic Clinical History & Physical Notes for Cerebral Ischemia
Muhammad Aftkhar
Grand Canyon University
December 04th, 2020
Academic Clinical History & Physical Notes for Cerebral Ischemia
I am presenting the academic clinical history and physical notes for the patient of ischemic stroke. Ischemic stroke or cerebral ischemia occurs when one of the cerebral arteries is blocked by the clot leading to diminished blood supply and oxygen to brain cells resulting in damage or death of brain cells (Celik et al., 2020)
History and Physical Note
1.Chief complaint/reason for admission/visit/consult.
A 52 years old male patient came to the acute care hospital with the chief complaint of sudden severe headache, dizziness, and slurred speech.
HPI for the H&P or consult notes.
The patient felt a severe burning and shooting pain in the frontal region of the head while he was reading the newspaper in the morning. The patient said that he developed blurred vision during reading. The patient felt numbness when the pain started (Harriot et al., 2020). The patient said that the pain was not subsiding with the time as it persisted since its onset. The pain scale was nine by 10, started in the frontal region, and radiated towards the temporal region. The associated symptoms with pain are nausea, vomiting, aphasia, dysarthria, apraxia, and vertigo (De Cock, et al., 2020). The symptoms become aggravate in a standing position and become alleviating when he lay down on the bed with 3 pillows. The patient felt a significant change in body posture. He is positive for facial drooping while negative for fever and chills. He finds difficulty in sitting and maintaining coordination. The patient stated that he had a medical history of neck trauma in a road accident. He was hospitalized for 3 weeks after neck surgery.
2.Medical, surgical, family, social, and allergy history.
Medical history
The patient has hypertension and hypercholesterolemia (Haegens, et al., 2018).
Surgical history
The patient underwent neck surgery after neck trauma at the age of 42.
Family history
The patient’s mother is alive and diabetic. The father of the patient died due to a cardiac stroke. His sister is normal. One of the two brothers has hypertension, and the other is normal. Currently, the patient is living with his normal wife.
Social history
The patient has a long history of smoking and boozing, coupled with a sedentary lifestyle.
Allergy history
· Raw fruits and vegetables, Shellfish, Soy.
· Amoxicillin and aspirin.
3.Home medications, including dosages, route, frequency, and current medications, if a consultation note.
Antihypertensive drugs Edarbi & Hygroton.
40 mg oral Edarbi once a day, as the patient is on diuretics, Hygroton. Oral 50 mg Hygroton once in the morning.
Hypercholesterolemic drugs Lipitor
Oral tablet 40 mg once a day. He takes this tablet at night.
4.Review of systems with all body systems for H&P or consult notes. Review of systems i ...
1
15
Academic Clinical History & Physical Notes for Cerebral Ischemia
Muhammad Aftkhar
Grand Canyon University
December 04th, 2020
Academic Clinical History & Physical Notes for Cerebral Ischemia
I am presenting the academic clinical history and physical notes for the patient of ischemic stroke. Ischemic stroke or cerebral ischemia occurs when one of the cerebral arteries is blocked by the clot leading to diminished blood supply and oxygen to brain cells resulting in damage or death of brain cells (Celik et al., 2020)
History and Physical Note
1.Chief complaint/reason for admission/visit/consult.
A 52 years old male patient came to the acute care hospital with the chief complaint of sudden severe headache, dizziness, and slurred speech.
HPI for the H&P or consult notes.
The patient felt a severe burning and shooting pain in the frontal region of the head while he was reading the newspaper in the morning. The patient said that he developed blurred vision during reading. The patient felt numbness when the pain started (Harriot et al., 2020). The patient said that the pain was not subsiding with the time as it persisted since its onset. The pain scale was nine by 10, started in the frontal region, and radiated towards the temporal region. The associated symptoms with pain are nausea, vomiting, aphasia, dysarthria, apraxia, and vertigo (De Cock, et al., 2020). The symptoms become aggravate in a standing position and become alleviating when he lay down on the bed with 3 pillows. The patient felt a significant change in body posture. He is positive for facial drooping while negative for fever and chills. He finds difficulty in sitting and maintaining coordination. The patient stated that he had a medical history of neck trauma in a road accident. He was hospitalized for 3 weeks after neck surgery.
2.Medical, surgical, family, social, and allergy history.
Medical history
The patient has hypertension and hypercholesterolemia (Haegens, et al., 2018).
Surgical history
The patient underwent neck surgery after neck trauma at the age of 42.
Family history
The patient’s mother is alive and diabetic. The father of the patient died due to a cardiac stroke. His sister is normal. One of the two brothers has hypertension, and the other is normal. Currently, the patient is living with his normal wife.
Social history
The patient has a long history of smoking and boozing, coupled with a sedentary lifestyle.
Allergy history
· Raw fruits and vegetables, Shellfish, Soy.
· Amoxicillin and aspirin.
3.Home medications, including dosages, route, frequency, and current medications, if a consultation note.
Antihypertensive drugs Edarbi & Hygroton.
40 mg oral Edarbi once a day, as the patient is on diuretics, Hygroton. Oral 50 mg Hygroton once in the morning.
Hypercholesterolemic drugs Lipitor
Oral tablet 40 mg once a day. He takes this tablet at night.
4.Review of systems with all body systems for H&P or consult notes. Review of systems i ...
1
15
Academic Clinical History & Physical Notes for Cerebral Ischemia
I am presenting the academic clinical history and physical notes for the patient of ischemic stroke. Ischemic stroke or cerebral ischemia occurs when one of the cerebral arteries is blocked by the clot leading to diminished blood supply and oxygen to brain cells resulting in damage or death of brain cells (Celik et al., 2020)
History and Physical Note
1.Chief complaint/reason for admission/visit/consult.
A 52 years old male patient came to the acute care hospital with the chief complaint of sudden severe headache, dizziness, and slurred speech.
HPI for the H&P or consult notes.
The patient felt a severe burning and shooting pain in the frontal region of the head while he was reading the newspaper in the morning. The patient said that he developed blurred vision during reading. The patient felt numbness when the pain started (Harriot et al., 2020). The patient said that the pain was not subsiding with the time as it persisted since its onset. The pain scale was nine by 10, started in the frontal region, and radiated towards the temporal region. The associated symptoms with pain are nausea, vomiting, aphasia, dysarthria, apraxia, and vertigo (De Cock, et al., 2020). The symptoms become aggravate in a standing position and become alleviating when he lay down on the bed with 3 pillows. The patient felt a significant change in body posture. He is positive for facial drooping while negative for fever and chills. He finds difficulty in sitting and maintaining coordination. The patient stated that he had a medical history of neck trauma in a road accident. He was hospitalized for 3 weeks after neck surgery.
2.Medical, surgical, family, social, and allergy history.
Medical history
The patient has hypertension and hypercholesterolemia (Haegens, et al., 2018).
Surgical history
The patient underwent neck surgery after neck trauma at the age of 42.
Family history
The patient’s mother is alive and diabetic. The father of the patient died due to a cardiac stroke. His sister is normal. One of the two brothers has hypertension, and the other is normal. Currently, the patient is living with his normal wife.
Social history
The patient has a long history of smoking and boozing, coupled with a sedentary lifestyle.
Allergy history
· Raw fruits and vegetables, Shellfish, Soy.
· Amoxicillin and aspirin.
3.Home medications, including dosages, route, frequency, and current medications, if a consultation note.
Antihypertensive drugs Edarbi & Hygroton.
40 mg oral Edarbi once a day, as the patient is on diuretics, Hygroton. Oral 50 mg Hygroton once in the morning.
Hypercholesterolemic drugs Lipitor
Oral tablet 40 mg once a day. He takes this tablet at night.
4.Review of systems with all body systems for H&P or consult notes. Review of systems is what the patient or family/friends tell you (by body system).
General appearance
The patient shows facial we ...
1
15
Academic Clinical History & Physical Notes for Cerebral Ischemia
I am presenting the academic clinical history and physical notes for the patient of ischemic stroke. Ischemic stroke or cerebral ischemia occurs when one of the cerebral arteries is blocked by the clot leading to diminished blood supply and oxygen to brain cells resulting in damage or death of brain cells (Celik et al., 2020)
History and Physical Note
1.Chief complaint/reason for admission/visit/consult.
A 52 years old male patient came to the acute care hospital with the chief complaint of sudden severe headache, dizziness, and slurred speech.
HPI for the H&P or consult notes.
The patient felt a severe burning and shooting pain in the frontal region of the head while he was reading the newspaper in the morning. The patient said that he developed blurred vision during reading. The patient felt numbness when the pain started (Harriot et al., 2020). The patient said that the pain was not subsiding with the time as it persisted since its onset. The pain scale was nine by 10, started in the frontal region, and radiated towards the temporal region. The associated symptoms with pain are nausea, vomiting, aphasia, dysarthria, apraxia, and vertigo (De Cock, et al., 2020). The symptoms become aggravate in a standing position and become alleviating when he lay down on the bed with 3 pillows. The patient felt a significant change in body posture. He is positive for facial drooping while negative for fever and chills. He finds difficulty in sitting and maintaining coordination. The patient stated that he had a medical history of neck trauma in a road accident. He was hospitalized for 3 weeks after neck surgery.
2.Medical, surgical, family, social, and allergy history.
Medical history
The patient has hypertension and hypercholesterolemia (Haegens, et al., 2018).
Surgical history
The patient underwent neck surgery after neck trauma at the age of 42.
Family history
The patient’s mother is alive and diabetic. The father of the patient died due to a cardiac stroke. His sister is normal. One of the two brothers has hypertension, and the other is normal. Currently, the patient is living with his normal wife.
Social history
The patient has a long history of smoking and boozing, coupled with a sedentary lifestyle.
Allergy history
· Raw fruits and vegetables, Shellfish, Soy.
· Amoxicillin and aspirin.
3.Home medications, including dosages, route, frequency, and current medications, if a consultation note.
Antihypertensive drugs Edarbi & Hygroton.
40 mg oral Edarbi once a day, as the patient is on diuretics, Hygroton. Oral 50 mg Hygroton once in the morning.
Hypercholesterolemic drugs Lipitor
Oral tablet 40 mg once a day. He takes this tablet at night.
4.Review of systems with all body systems for H&P or consult notes. Review of systems is what the patient or family/friends tell you (by body system).
General appearance
The patient shows facial we ...
This is a review of a case of an infant admitted to pediatric ICU as a case of epidural hematoma after traumatic brain injury. A brief summary of the most important aspects. Part of the residency teaching program for pediatric residents at the pediatric and neonatology department at Istishari Arab Hospital, Ramallah, Palestine.
1. Initial assessment and management of the trauma patient.pptxWalterBenites2
La primera etapa del curso ATLS (Advanced Trauma Life Support) se conoce como "Evaluación Inicial". En esta etapa, los estudiantes de medicina aprenden un enfoque sistemático y estructurado para evaluar a un paciente traumatizado de manera rápida y eficaz.
La Evaluación Inicial se centra en identificar y abordar de inmediato las lesiones que amenazan la vida del paciente.
Antibiotic Stewardship by Anushri Srivastava.pptxAnushriSrivastav
Stewardship is the act of taking good care of something.
Antimicrobial stewardship is a coordinated program that promotes the appropriate use of antimicrobials (including antibiotics), improves patient outcomes, reduces microbial resistance, and decreases the spread of infections caused by multidrug-resistant organisms.
WHO launched the Global Antimicrobial Resistance and Use Surveillance System (GLASS) in 2015 to fill knowledge gaps and inform strategies at all levels.
ACCORDING TO apic.org,
Antimicrobial stewardship is a coordinated program that promotes the appropriate use of antimicrobials (including antibiotics), improves patient outcomes, reduces microbial resistance, and decreases the spread of infections caused by multidrug-resistant organisms.
ACCORDING TO pewtrusts.org,
Antibiotic stewardship refers to efforts in doctors’ offices, hospitals, long term care facilities, and other health care settings to ensure that antibiotics are used only when necessary and appropriate
According to WHO,
Antimicrobial stewardship is a systematic approach to educate and support health care professionals to follow evidence-based guidelines for prescribing and administering antimicrobials
In 1996, John McGowan and Dale Gerding first applied the term antimicrobial stewardship, where they suggested a causal association between antimicrobial agent use and resistance. They also focused on the urgency of large-scale controlled trials of antimicrobial-use regulation employing sophisticated epidemiologic methods, molecular typing, and precise resistance mechanism analysis.
Antimicrobial Stewardship(AMS) refers to the optimal selection, dosing, and duration of antimicrobial treatment resulting in the best clinical outcome with minimal side effects to the patients and minimal impact on subsequent resistance.
According to the 2019 report, in the US, more than 2.8 million antibiotic-resistant infections occur each year, and more than 35000 people die. In addition to this, it also mentioned that 223,900 cases of Clostridoides difficile occurred in 2017, of which 12800 people died. The report did not include viruses or parasites
VISION
Being proactive
Supporting optimal animal and human health
Exploring ways to reduce overall use of antimicrobials
Using the drugs that prevent and treat disease by killing microscopic organisms in a responsible way
GOAL
to prevent the generation and spread of antimicrobial resistance (AMR). Doing so will preserve the effectiveness of these drugs in animals and humans for years to come.
being to preserve human and animal health and the effectiveness of antimicrobial medications.
to implement a multidisciplinary approach in assembling a stewardship team to include an infectious disease physician, a clinical pharmacist with infectious diseases training, infection preventionist, and a close collaboration with the staff in the clinical microbiology laboratory
to prevent antimicrobial overuse, misuse and abuse.
to minimize the developme
Telehealth Psychology Building Trust with Clients.pptxThe Harvest Clinic
Telehealth psychology is a digital approach that offers psychological services and mental health care to clients remotely, using technologies like video conferencing, phone calls, text messaging, and mobile apps for communication.
The dimensions of healthcare quality refer to various attributes or aspects that define the standard of healthcare services. These dimensions are used to evaluate, measure, and improve the quality of care provided to patients. A comprehensive understanding of these dimensions ensures that healthcare systems can address various aspects of patient care effectively and holistically. Dimensions of Healthcare Quality and Performance of care include the following; Appropriateness, Availability, Competence, Continuity, Effectiveness, Efficiency, Efficacy, Prevention, Respect and Care, Safety as well as Timeliness.
We understand the unique challenges pickleball players face and are committed to helping you stay healthy and active. In this presentation, we’ll explore the three most common pickleball injuries and provide strategies for prevention and treatment.
CRISPR-Cas9, a revolutionary gene-editing tool, holds immense potential to reshape medicine, agriculture, and our understanding of life. But like any powerful tool, it comes with ethical considerations.
Unveiling CRISPR: This naturally occurring bacterial defense system (crRNA & Cas9 protein) fights viruses. Scientists repurposed it for precise gene editing (correction, deletion, insertion) by targeting specific DNA sequences.
The Promise: CRISPR offers exciting possibilities:
Gene Therapy: Correcting genetic diseases like cystic fibrosis.
Agriculture: Engineering crops resistant to pests and harsh environments.
Research: Studying gene function to unlock new knowledge.
The Peril: Ethical concerns demand attention:
Off-target Effects: Unintended DNA edits can have unforeseen consequences.
Eugenics: Misusing CRISPR for designer babies raises social and ethical questions.
Equity: High costs could limit access to this potentially life-saving technology.
The Path Forward: Responsible development is crucial:
International Collaboration: Clear guidelines are needed for research and human trials.
Public Education: Open discussions ensure informed decisions about CRISPR.
Prioritize Safety and Ethics: Safety and ethical principles must be paramount.
CRISPR offers a powerful tool for a better future, but responsible development and addressing ethical concerns are essential. By prioritizing safety, fostering open dialogue, and ensuring equitable access, we can harness CRISPR's power for the benefit of all. (2998 characters)
QA Paediatric dentistry department, Hospital Melaka 2020Azreen Aj
QA study - To improve the 6th monthly recall rate post-comprehensive dental treatment under general anaesthesia in paediatric dentistry department, Hospital Melaka
R3 Stem Cells and Kidney Repair A New Horizon in Nephrology.pptxR3 Stem Cell
R3 Stem Cells and Kidney Repair: A New Horizon in Nephrology" explores groundbreaking advancements in the use of R3 stem cells for kidney disease treatment. This insightful piece delves into the potential of these cells to regenerate damaged kidney tissue, offering new hope for patients and reshaping the future of nephrology.
Defecation
Normal defecation begins with movement in the left colon, moving stool toward the anus. When stool reaches the rectum, the distention causes relaxation of the internal sphincter and an awareness of the need to defecate. At the time of defecation, the external sphincter relaxes, and abdominal muscles contract, increasing intrarectal pressure and forcing the stool out
The Valsalva maneuver exerts pressure to expel faeces through a voluntary contraction of the abdominal muscles while maintaining forced expiration against a closed airway. Patients with cardiovascular disease, glaucoma, increased intracranial pressure, or a new surgical wound are at greater risk for cardiac dysrhythmias and elevated blood pressure with the Valsalva maneuver and need to avoid straining to pass the stool.
Normal defecation is painless, resulting in passage of soft, formed stool
CONSTIPATION
Constipation is a symptom, not a disease. Improper diet, reduced fluid intake, lack of exercise, and certain medications can cause constipation. For example, patients receiving opiates for pain after surgery often require a stool softener or laxative to prevent constipation. The signs of constipation include infrequent bowel movements (less than every 3 days), difficulty passing stools, excessive straining, inability to defecate at will, and hard feaces
IMPACTION
Fecal impaction results from unrelieved constipation. It is a collection of hardened feces wedged in the rectum that a person cannot expel. In cases of severe impaction the mass extends up into the sigmoid colon.
DIARRHEA
Diarrhea is an increase in the number of stools and the passage of liquid, unformed feces. It is associated with disorders affecting digestion, absorption, and secretion in the GI tract. Intestinal contents pass through the small and large intestine too quickly to allow for the usual absorption of fluid and nutrients. Irritation within the colon results in increased mucus secretion. As a result, feces become watery, and the patient is unable to control the urge to defecate. Normally an anal bag is safe and effective in long-term treatment of patients with fecal incontinence at home, in hospice, or in the hospital. Fecal incontinence is expensive and a potentially dangerous condition in terms of contamination and risk of skin ulceration
HEMORRHOIDS
Hemorrhoids are dilated, engorged veins in the lining of the rectum. They are either external or internal.
FLATULENCE
As gas accumulates in the lumen of the intestines, the bowel wall stretches and distends (flatulence). It is a common cause of abdominal fullness, pain, and cramping. Normally intestinal gas escapes through the mouth (belching) or the anus (passing of flatus)
FECAL INCONTINENCE
Fecal incontinence is the inability to control passage of feces and gas from the anus. Incontinence harms a patient’s body image
PREPARATION AND GIVING OF LAXATIVESACCORDING TO POTTER AND PERRY,
An enema is the instillation of a solution into the rectum and sig
Leading the Way in Nephrology: Dr. David Greene's Work with Stem Cells for Ki...Dr. David Greene Arizona
As we watch Dr. Greene's continued efforts and research in Arizona, it's clear that stem cell therapy holds a promising key to unlocking new doors in the treatment of kidney disease. With each study and trial, we step closer to a world where kidney disease is no longer a life sentence but a treatable condition, thanks to pioneers like Dr. David Greene.
CHAPTER 1 SEMESTER V PREVENTIVE-PEDIATRICS.pdfSachin Sharma
This content provides an overview of preventive pediatrics. It defines preventive pediatrics as preventing disease and promoting children's physical, mental, and social well-being to achieve positive health. It discusses antenatal, postnatal, and social preventive pediatrics. It also covers various child health programs like immunization, breastfeeding, ICDS, and the roles of organizations like WHO, UNICEF, and nurses in preventive pediatrics.
2023_Sp_Neuro Case Study_Acute Intracranial Problems-1.pptx
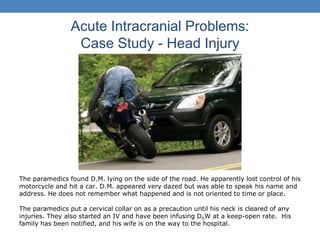
1. Acute Intracranial Problems:
Case Study - Head Injury
The paramedics found D.M. lying on the side of the road. He apparently lost control of his
motorcycle and hit a car. D.M. appeared very dazed but was able to speak his name and
address. He does not remember what happened and is not oriented to time or place.
The paramedics put a cervical collar on as a precaution until his neck is cleared of any
injuries. They also started an IV and have been infusing D5W at a keep-open rate. His
family has been notified, and his wife is on the way to the hospital.
2. Vital signs were taken right before he was brought into
the emergency department. His BP was 118/72, his
heart rate was 68, and his respiratory rate was 16.
His lungs were clear and he was in normal sinus
rhythm on the monitor.
5. “I have a terrible headache and feel sick to my stomach.
Maybe it’s a 10… I just don’t know.
Question: Would the nurse give pain medication?
6. Continued assessment-2
Nurse asks patient to look at her. “Can you hear
me?” His response is not understandable.
When painful stimulus is applied, he withdraws
his arm, and opens his eyes. He groans.
7. Glasgow Coma Scale
• What would you give this patient based on the latest
assessment findings following the change in his LOC?
8. Deteriorating Condition
The right side of his head is swollen and boggy.
He has bruising and ecchymosis behind his ear.
He opens eyes to painful stimuli (pressing on
sternum). He has clear drainage from his ear.
What could this indicate?
10. Early, Moderate, Late Signs of Increased ICP
Early: Decreased LOC
Moderate: H/A, sudden
vomiting without nausea
Late: Irregular respirations such as Cheyne Stokes, eyes with pupils fixed, dilated or
unequal. Normal is 2-6. Doll’s eyes + is normal. Babinski Reflex +: toes fan out when
stroked
Very Late and Deadly: Cushing's triad: widening of PP, decreased HR, deceased
respirations (irregular)
Very Late: Seizures, coma, abnormal posturing; decorticate and decerebrate.
11. Question: What are other signs of
increased ICP?
A. Altered respiratory pattern
B. Dilation of the ipsilateral pupil with sluggish or no response to light
C. Increased systolic pressure
D. Contralateral hemiparesis
E. Decreasing heart rate
F. Vomiting
G. Weak, thready pulse
H. Change in level of consciousness
I. Blurred or double vision
12. What is a priority for the nurse to
implement immediately?
A. apply oxygen via nasal cannula.
B. position the patient with his head elevated.
C. call the radiology department for a stat skull x-
ray.
D. Call HCP for intubation.
13. NCLEX Question:
A. Lower the HOB to 20 degrees.
B. B. Get MRI stat
C. C. Give atropine IV
D. D. Get C-Spine and CT
A client is found lying on the floor with bleeding at
the back of the head. HR is 45, BP is 220/88. What
is first action by the nurse?
14. NCLEX Question
A. Grips are equal and strong.
B. Toes fan out when the sole is stoked.
C. Eyes move in opposite direction when
patient’s head is turned from side to side.
D. Extremities contract to the core
E. Pupils are fixed at 8 mm.
F. LOC stays the same, without changes.
The client has sustained a head injury. Which of the
following signs are positive (not deteriorating)
assessment findings? (SATA)
15. A linear skull fracture and subdural hematoma is
evident from CT and skull xrays.
16. Matching
A. Administration of 100%
oxygen
B. Elevation of head of bed to 30
degrees
C. Endotracheal intubation and
mechanical ventilation
1. Maintains airway and ventilation
2. Ensures adequate oxygenation to
support brain function
3. Promotes venous drainage from
the brain
What interventions go with
rationales for reducing ICP?
19. Post OP Orders:
•ICP monitor
•Ventricular catheter
•Arterial catheter
•Cardiac monitoring
•ET tube with mechanical ventilation
•Head dressing
•NS at 75 mL/hr
•NG tube to suction
•Measure ICP hourly
•HOB elevate 30-45 degrees
20. ICP
Brain, blood, CSF must stay balanced to keep ICP WNL
Influencing factors: arterial and venous pressure, intraabdominal and intrathoracic pressure, posture, temperature and
blood gases especially CO2.
ICP: 5-15; > 20 is abnormal
CPP: amount of pressure needed to maintain adequate brain blood flow;
CPP = MAP – ICP
Normal: 60-100
Less than 50 = ischemia and tissue death
Mean arterial pressure (MAP): 70 is lower limit before symptoms develop (syncope, blurred vision) and 150 is upper
limit (severe vasoconstriction); see page 1301 in Lewis
PaCO2 increases leads to vasodilation and increased CBF (cranial blood flow), decreased PaCO2 leads to
vasoconstriction and decrease CBF. PaO2 < 50 mm Hg leads to dilation and increases CBF. So want to keep PaO2 at
or greater than 100. See pg 1302.
ICP
22. Positioning the ICP
Drainage System
Question: You review the hospital's procedure
for draining cerebrospinal fluid (CSF) via the
external ventricular drain in case D.M.'s ICP
increases to the point of needing acute
intervention. Upon review of the procedure,
you identify that the drip chamber and
drainage bag should be placed at the level of
the patient's ventricular reference point,
approximating the foramen of Monroe. A
reference point for this foramen is
the _______________ of the ear.
23. Clinical Manifestations: Increased ICP
• Change in LOC – most sensitive
(subtle to coma)
• VS change: Example
8 AM: 150/86, P-84, R-14
10 AM: 166/74, P-54, RR-10
to16
• Ocular: Optic II, Oculomotor III,
trochlear IV, abducens VI
• Motor: contralateral hemiparesis or
hemiplegia; posturing
• Headache: Pain at night or
morning is worse; straining
increases pain.
• Vomiting: unexpected, projectile
w/o nausea preceding.
25. Assessment Findings
• Patient Data: C/o increasing headache. Drowsy,
confused. Ptosis of the left eye and weakness on the right
side.
• How would you assess for drift with the patient in bed?
30. ICP Measurements
The first ICP measurement is 10 mm Hg. Your first action
should be to do which of the following?
A. Document findings and continue with planned care.
B. Notify the physician of the elevated ICP.
C. Lower the HOB to increase cranial perfusion pressure.
D. Increase the elevation of the HOB from 30 to 45
degrees.
31. Ventriculostomy for ICP
Keep SBP 100-160 and CPP > 60 mm Hg
Normal CPP is 60-100 (Lewis, pg. 1301)
If BP 120/70 and ICP is 20, what is CPP?
If CPP is not normal, what interventions would you
consider?
32. Which Factors Lead to ^ ICP?
A. Coughing and sneezing.
B. Deep breathing
C. Endotracheal suctioning
D. Extreme hip and neck flexion
E. Fear and anxiety
F. Head of bed at 30 degrees.
G. Lateral positioning
H. PaCO2 of 52 mm Hg
I. PaO2 of 80 mm Hg
J. Pain
33. Delegating Activities
Which of the following activities could you delegate to an
unlicensed assistive personnel?
A. assess the ICP readings on another stable post op
patient.
B. Record intake and output on a post-op patient.
C. Teach another patient's family about the plan of care for
the day.
D. Evaluate the effect of an antianxiety agent on a patient
with a CVA.
34. Medications
Which of the following medications may be appropriate to
give this patient and why? (Select all that apply)
A. ranitidine (Zantac), famotidine (Pepcid)
B. mannitol (Osmitrol)
C. phenytoin (Dilantin)
D. D5W IV fluid
E. D5/1/4 NS IV fluid
F. Desmopressin (DDAVP ) or vasopressin (Pitressin)
36. Labs and Nursing Interventions
Lab results:
Na+ 140 mEq/L , K+ 4.6 mEq/L , Cl- 100 mEq/L , WBCs
17,000/µL, Hgb 13.9 g/dL , and Hct 40%.
ABGs: pH 7.43, PaO2 98 mm Hg, PaCO2 35 mm Hg, HCO3
23 mEq/L, SaO2 98%.
Based on these results, you would notify the physician
and do which of the following?
A. Ask for IV solution change.
B. Ask for drugs to lower ICP
C. Ask to decrease the RR and volume on the ventilator
D. Check the site and odor of head dressings.
38. What response should you give when
the wife asks specific questions about
his recovery?
A. Unfortunately, patients who have this type of brain trauma will always have
some degree of neurologic impairment.
B. He will require long-term rehabilitation for motor and sensory losses
before he can function normally and return home.
C. He will be expected to show gradual, continuous improvement in
neurologic function until he has returned to normal status.
D. Recovery is very individualized and may continue for 6 months or longer
before a plateau is reached and a prognosis for recovery can be made.
39. Question:
What assessment finding requires immediate intervention
if found while a patient is receiving Mannitol?*
A. An ICP of 10 mmHg
B. Crackles throughout lung fields
C. BP 110/72
D. Patient complains of dry mouth and thirst
40. Question
Which of the following is contraindicated in
a patient with increased ICP?
A. Lumbar puncture
B. Midline position of the head
C. Hyperosmotic diuretics
D. Barbiturates medications
41. Question:
During the eye assessment of a patient with increased
ICP, you need to assess the oculocephalic reflex. If the
patient has brain stem damage what response will you
find?*
A. The eyes will roll down as the head is moved side to
side.
B. The eyes will move in the opposite direction as the
head is moved side to side.
C. The eyes will roll back as the head is moved side to
side.
D. The eyes will be in a fixed mid-line position as the
head is moved side to side.
42. Question
You’re maintaining an external ventricular drain. The ICP
readings should be?
A. 5 to 15 mmHg
B. 20 to 35 mmHg
C. 60 to 100 mmHg
D. 5 to 25 mmHg