Download to read offline

Chapter 3 of the outpatient coding and reporting guidelines emphasizes the correct usage of first-listed diagnoses in various outpatient scenarios, including surgery and routine medical visits. It highlights specific coding for chronic diseases, unconfirmed diagnoses, and various status codes, detailing how to categorize encounters appropriately. Additionally, it includes procedural coding requirements and guidelines for documenting patient conditions to ensure accurate and comprehensive reporting.
Introduction to Chapter 3 of ICD-10-CM Outpatient Coding, covering key topics and guidelines.
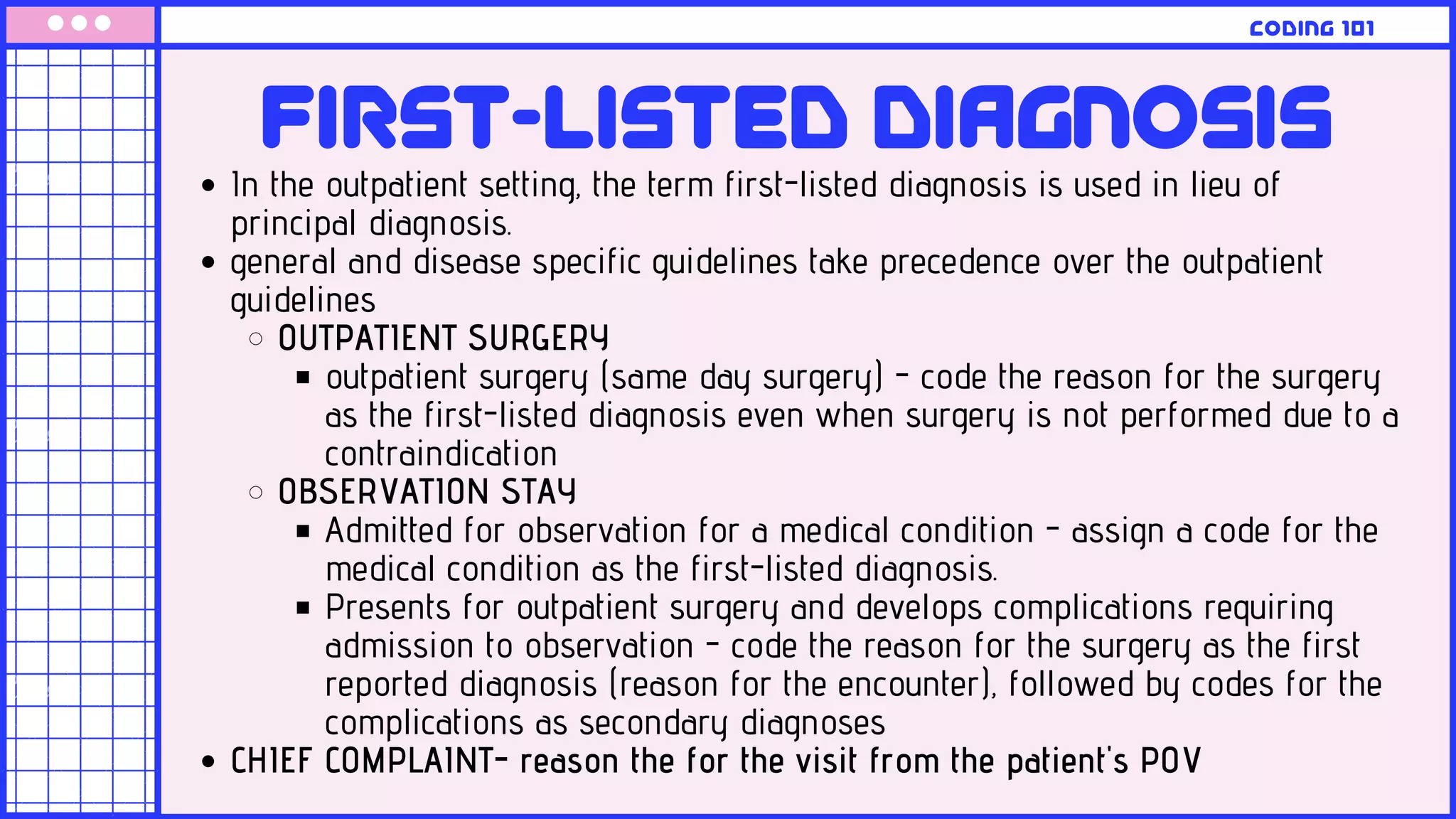
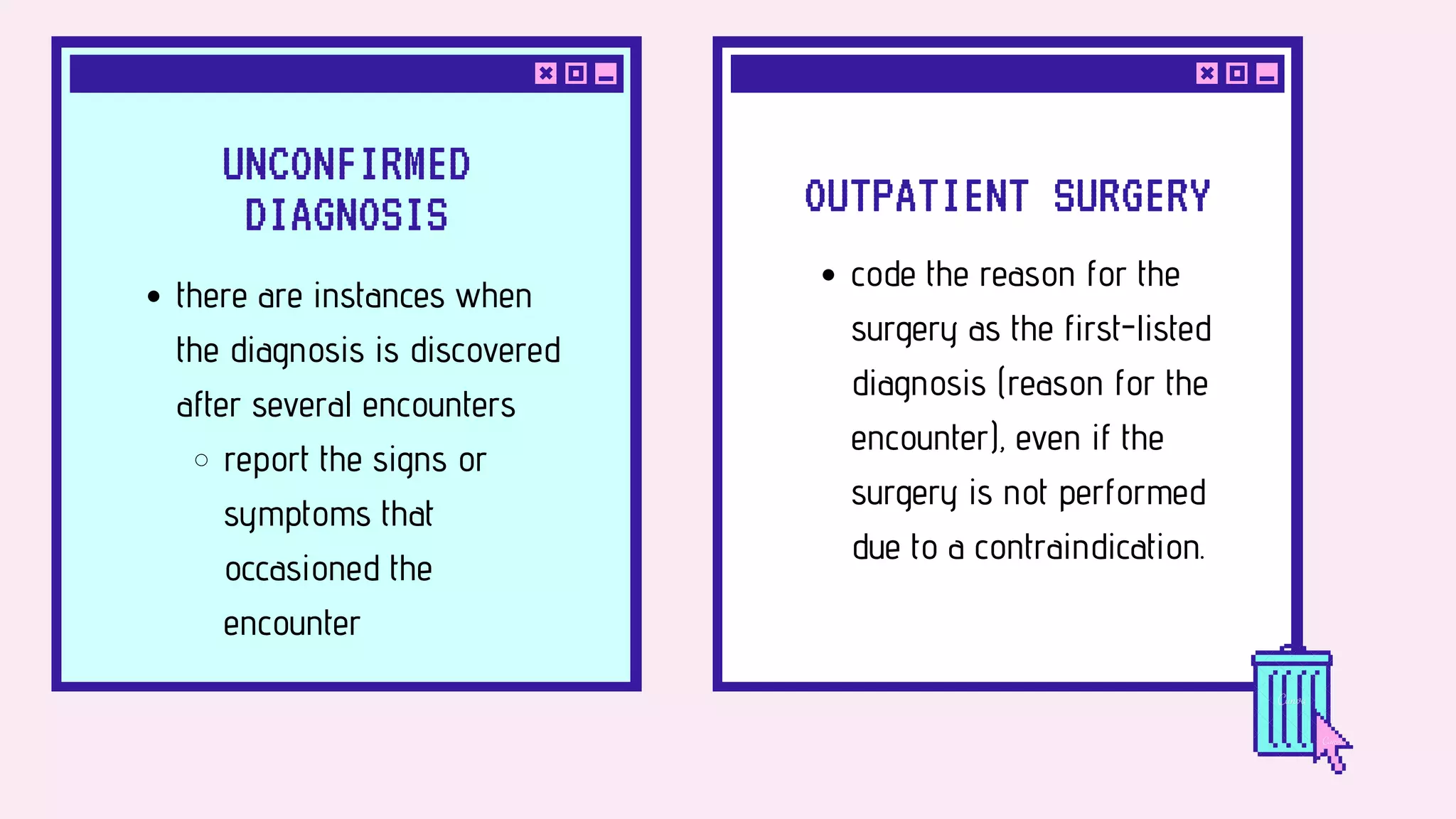
Focus on defining first-listed diagnosis and its application in outpatient surgery and unconfirmed diagnoses.
Details on coding additional diagnoses using specific codes, including Z-codes for exposure and preventive care.
Explanation of various status codes used in encounters, their significance, and examples including DNR and allergies.
Information on using the External Cause Index for coding environmental events and circumstances with Z-codes.
Guidance on listing first diagnoses, handling uncertainties, and coding chronic and documented conditions.
Focus on coding for therapeutic services, preoperative visits, and prenatal care in outpatient settings.



































































