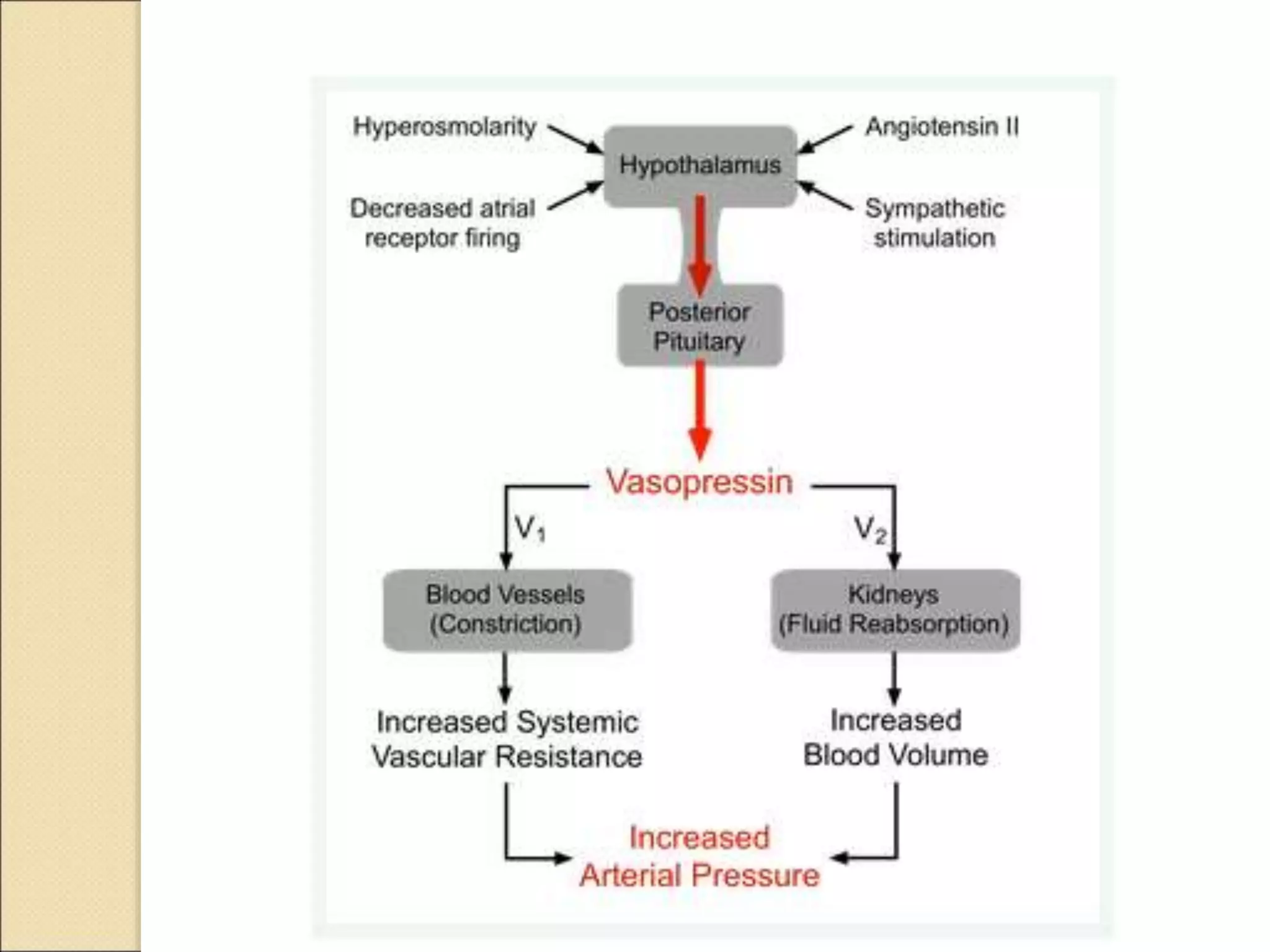
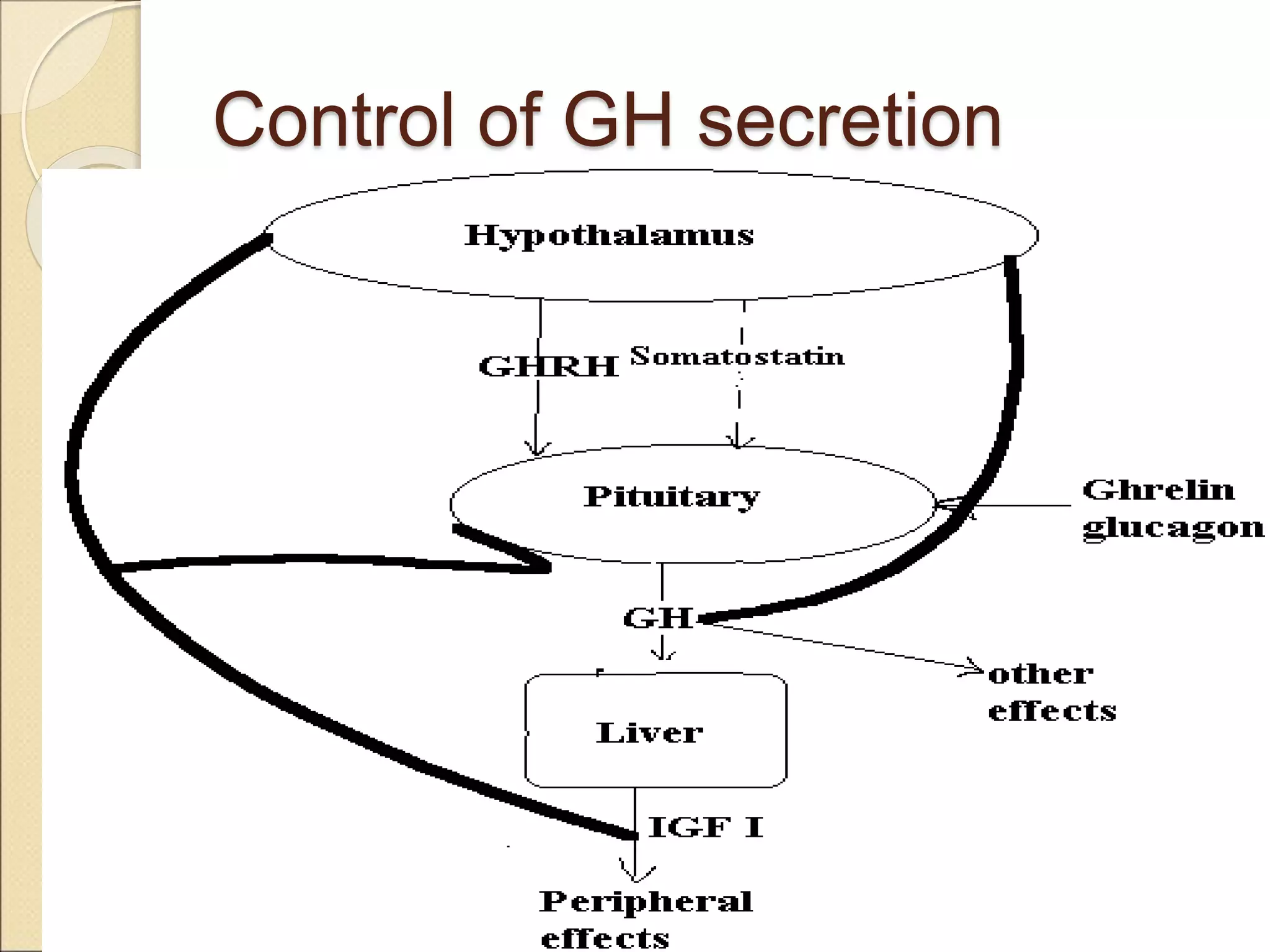
The document describes the relationship between the hypothalamus and pituitary gland. It discusses how the hypothalamus regulates the pituitary through releasing and inhibiting factors that control secretion of anterior pituitary hormones. The pituitary has anterior and posterior lobes, with the anterior secreting hormones that regulate growth, metabolism, and reproduction and the posterior secreting vasopressin and oxytocin which regulate water balance and milk letdown. The hypothalamus and pituitary form a complex regulatory system that controls many other endocrine glands.













































![African Pygmies
They have a normal GH level and a modest
decrease in plasma level of GHBP
Plasma [IGF I] fails to increase at the time
of puberty
However, they experience less growth than
non pygmy controls throughout the pre
pubertal period
Explanation for short stature is still
unsettled](https://image.slidesharecdn.com/hypothalamuspituitaryaxis-230309032629-d2740bf9/75/Hypothalamus-Pituitary-Axis-ppt-76-2048.jpg)












































![HYPOTHALAMIC AND PITUITARY HORMONES [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamicandpituitaryhormonesautosaved-240606131535-7cfeb320-thumbnail.jpg?width=640&height=640&fit=bounds)
































