Download as PDF, PPTX




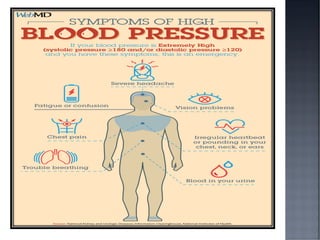
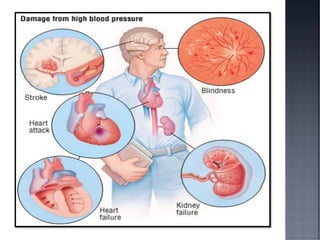

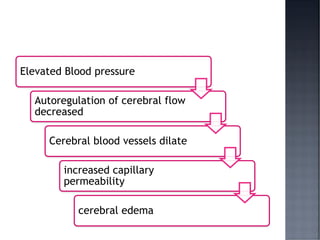
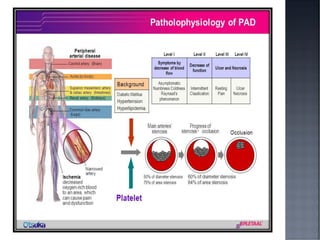
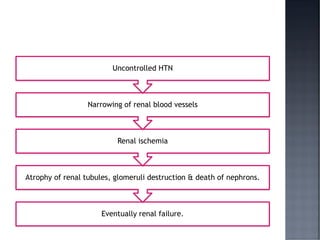
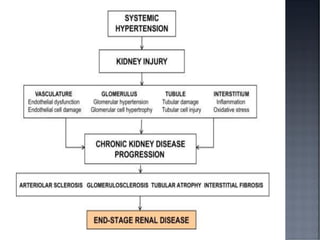











This document discusses hypertension (HTN), defining it as a persistent systolic blood pressure (SBP) of 130 mm Hg or more or diastolic blood pressure (DBP) of 80 mm Hg or more. Approximately 1.13 billion people worldwide have HTN, including 100-110 million people in India. HTN can lead to numerous complications affecting the heart, brain, kidneys and eyes if not properly managed. The document outlines assessment approaches for HTN, including medical history, physical examination, and lab tests to identify secondary causes and target organ damage from high blood pressure.























































































