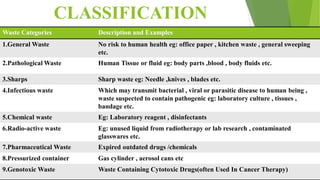
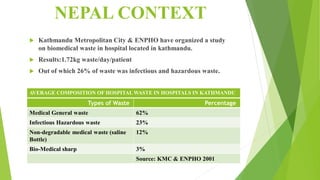
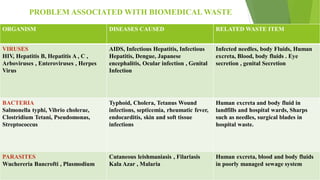
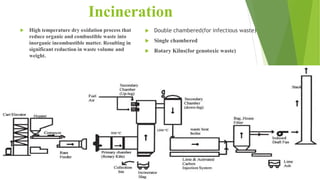
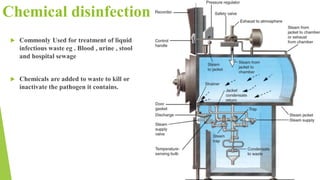
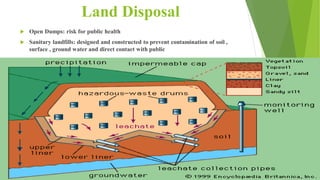
The document outlines hospital waste management practices, emphasizing the classification, generation, and treatment of healthcare waste, particularly in the context of Nepal. It categorizes waste types, noting that 75-90% is non-hazardous, while 10-15% is hazardous, and discusses the problems associated with improper disposal, including the risk of infectious diseases. It also highlights various treatment and disposal methods, such as incineration and chemical disinfection, and stresses the importance of proper segregation, storage, and transportation of healthcare waste.