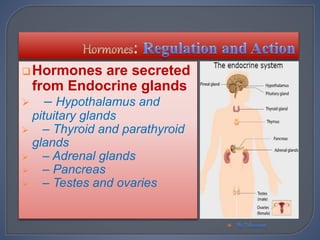
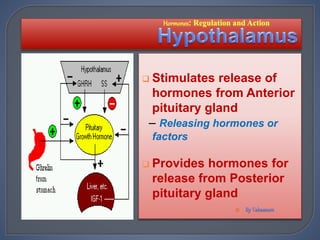
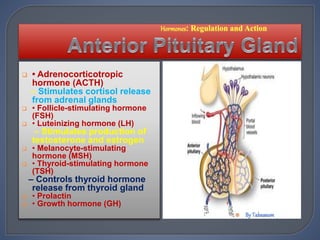
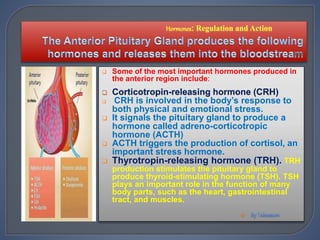
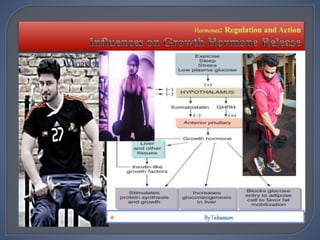
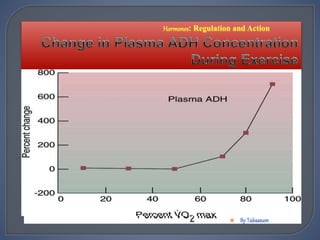
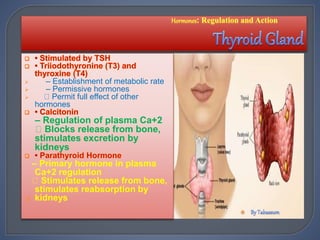
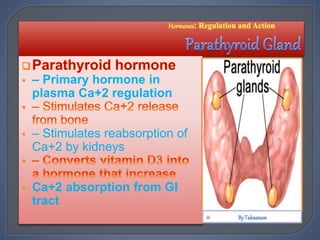
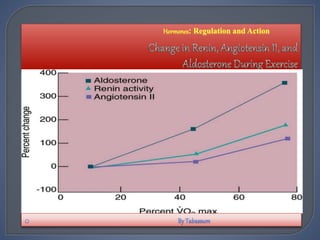
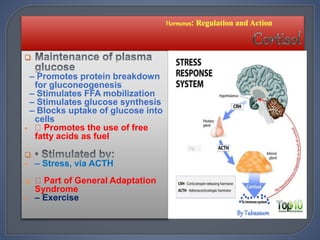
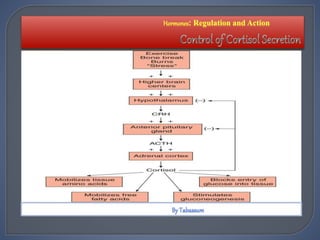
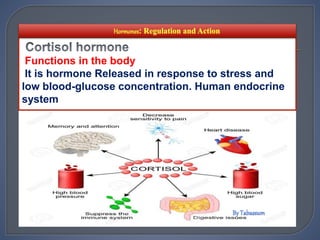
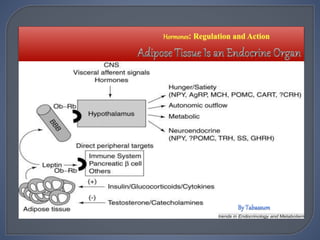
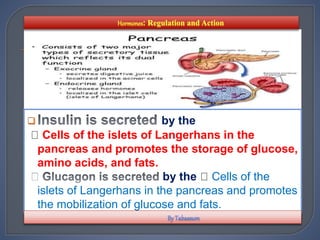
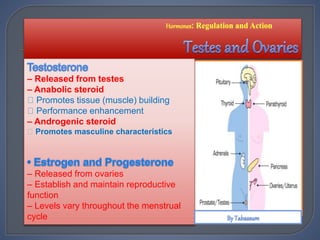
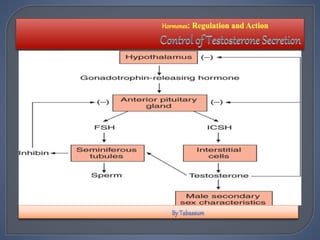
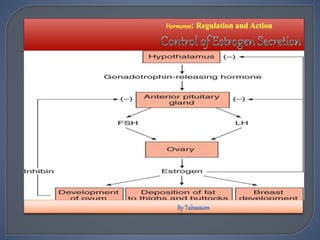
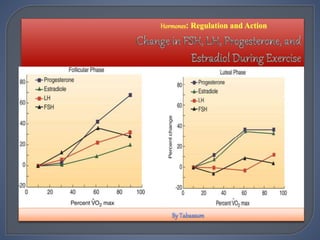
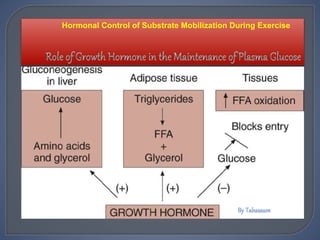
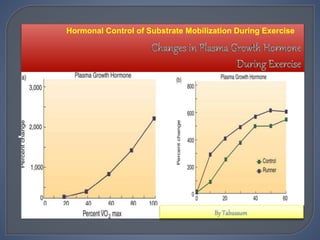
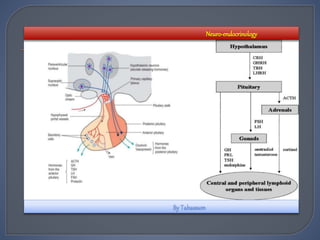
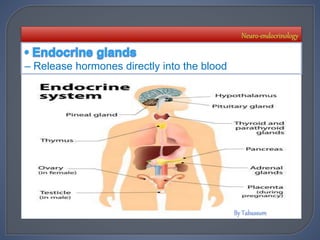
The document discusses the role of various endocrine glands in hormone regulation and response to exercise. It describes how the hypothalamus and pituitary gland control other glands like the thyroid, parathyroid, adrenal, pancreas and ovaries/testes to regulate functions. It also examines the hormonal response to acute and chronic exercise, noting increases in hormones like cortisol and ACTH with high intensity or prolonged exercise. Finally, it explores factors that can influence exercise-induced hormonal changes and the potential effects of long-term training.