Download to read offline
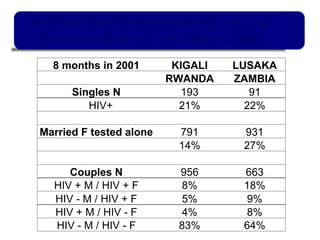

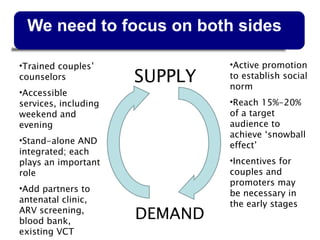

- The document discusses strategies for HIV testing of couples in sub-Saharan Africa, where most new infections occur within marriages. It highlights examples from Rwanda and Zambia where stand-alone and integrated testing of couples at antenatal clinics identified thousands of discordant couples. - Sustaining couples testing requires addressing both supply of testing services and demand through community promotion to establish it as a social norm. It takes testing 15-20% of target couples to achieve this. Incentives for transport and clinic promoters may be initially needed.



























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

