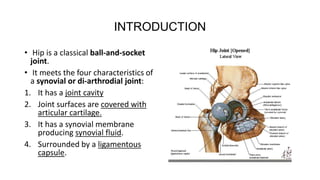
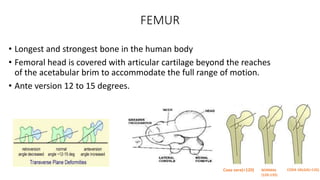
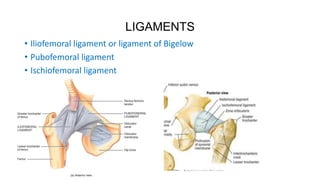
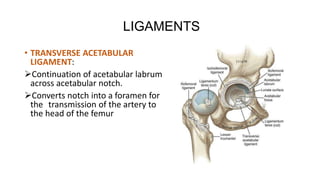
The document provides information on the anatomy, biomechanics, and principles of the hip joint. It describes the hip joint as a ball-and-socket synovial joint with articular cartilage covering the femoral head and acetabulum. Key ligaments that support the hip joint are also outlined. Biomechanics concepts like lever arms, forces, and strategies to reduce joint reaction forces are discussed. The principles of total hip replacement to decrease forces on the implant through acetabular deepening and increasing the abductor lever arm are presented.







![Anatomy and biomechanics of hip joint [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anatomyandbiomechanicsofhipjointautosaved-210831212052-thumbnail.jpg?width=640&height=640&fit=bounds)



























































