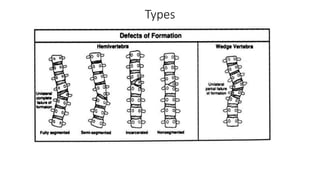
Hemivertebra is a condition where half of a vertebra fails to form, which can cause spinal deformities like scoliosis. It occurs in about 0.1-1% of live births and is more common in females. Hemivertebrae are the most frequent cause of congenital spinal deformity. The type and location of the hemivertebra can affect the degree and progression of the spinal deformity as the child grows. Treatment may involve early surgery to resect the hemivertebra and perform spinal fusion to correct the deformity and prevent further progression.