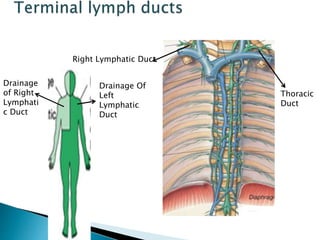
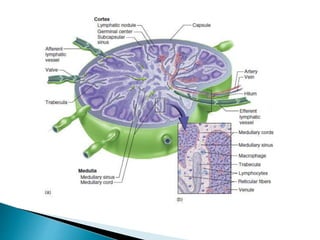
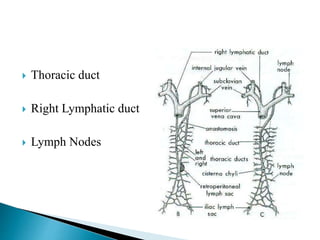
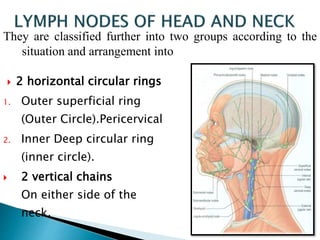
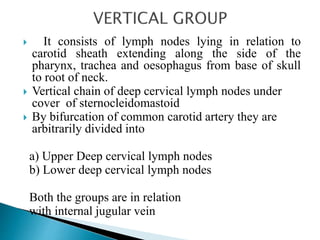
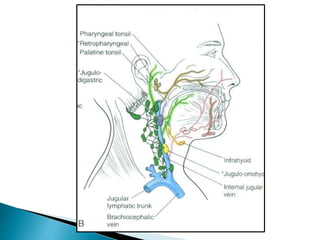
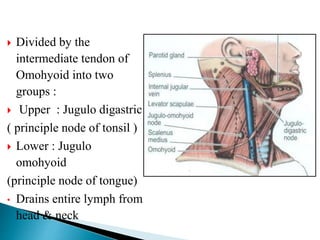
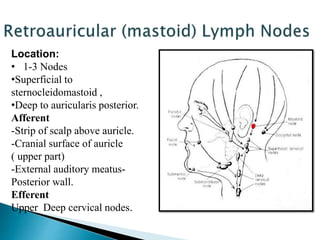
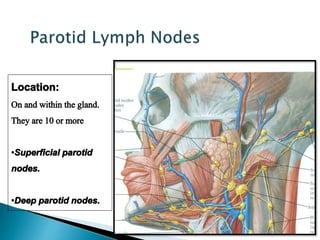
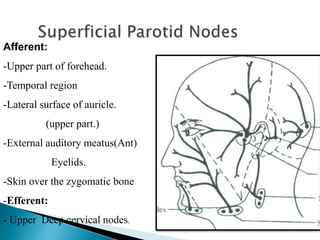
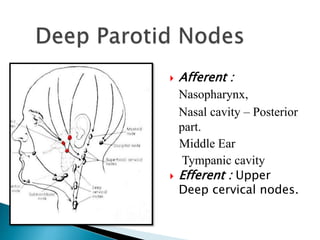
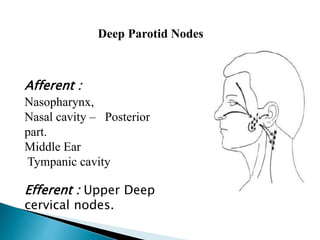
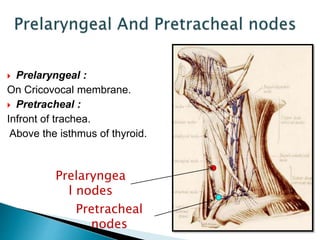
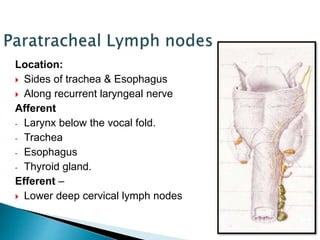
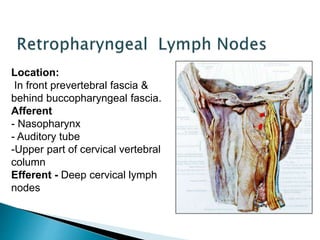
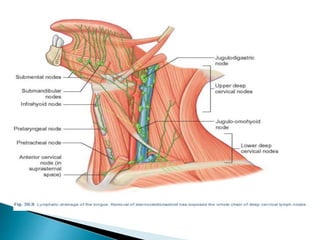
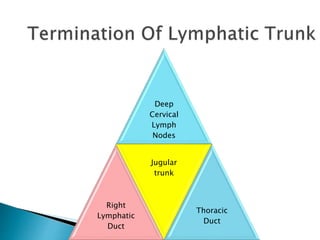
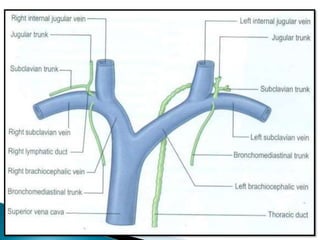
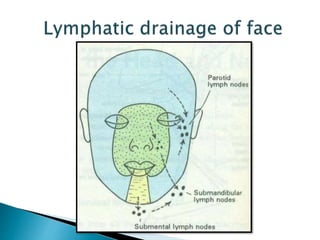
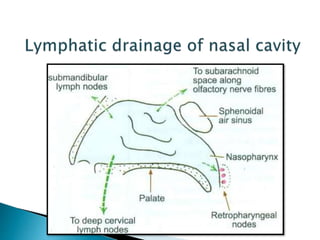
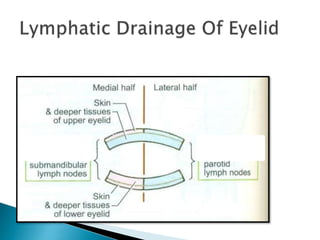
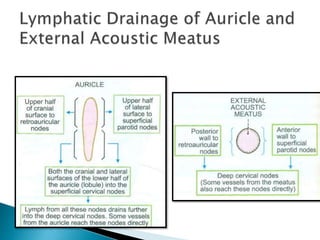
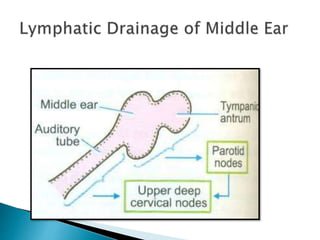
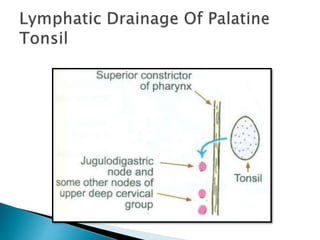
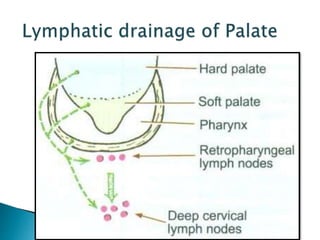
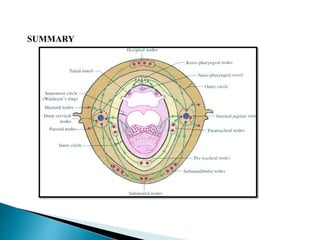
The document provides an overview of the lymphatic system, including its historical perspectives, embryological development, functions, anatomy, and clinical applications. It describes the key components and their roles, such as lymph, lymphatic vessels, lymph nodes, and lymphatic organs. The summary focuses on lymphatic drainage patterns in the head and neck region, noting that lymph drains from tissues and lymph nodes into the right lymphatic duct or thoracic duct. It also discusses the functions of lymph nodes in filtering pathogens and alerting the immune system.