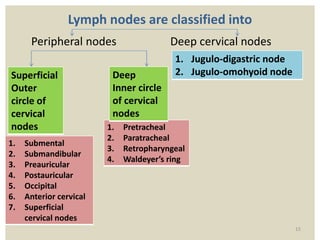
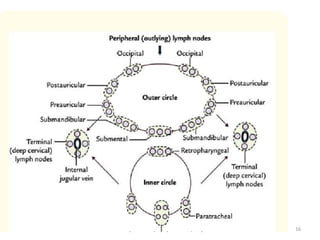
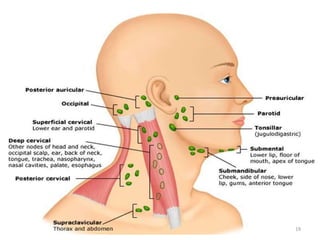
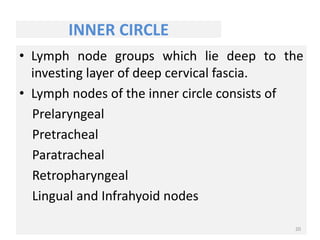
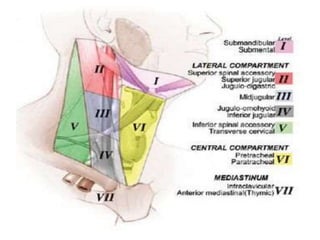
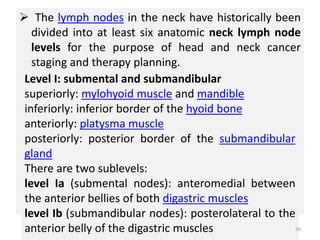
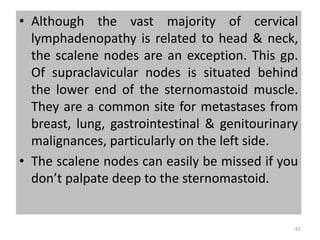
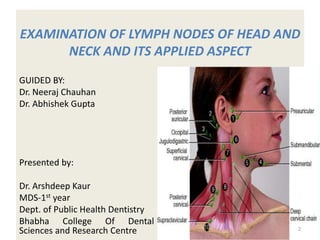
Lymph nodes in the head and neck can be examined and classified into different levels. There are about 300 lymph nodes in the head and neck region organized into two circles - the outer and inner circles. The outer circle includes submental, submandibular, preauricular and occipital nodes. The inner circle includes prelaryngeal, pretracheal, paratracheal and retropharyngeal nodes. Lymph nodes are further classified into 6 levels from I to VI based on their location for cancer staging and treatment planning. Lymph nodes examine antigen filtration and immune response initiation making examination important for clinical assessment.





![Path of lymph flow through a lymph node
Afferent lymphatics carry [afferent to bring to] lymph to the
lymph node from peripheral tissues. The afferent lymphatics
penetrate the capsule of the lymph node on the side opposite
to hilum.
The afferent vessels deliver lymph to the subcapsular space, a
meshwork of reticular fibers, macrophages, and dendritic cells.
Dendritic cells are involved in the initiation of immune
response.
Lymph next flow into the outer cortex , which contains B cells
with germinal centers that resemble those of lymphoid nodule.
11](https://image.slidesharecdn.com/lnheadandneck-230217054454-2b8ac3fa/85/LN-HEAD-AND-NECK-pptx-11-320.jpg)
![Lymph then flows through lymph sinuses in the deep cortex,
which is dominated by T cells.
Efferent lymphatics [efferent to bring out] leave the lymph node
at the hilum. These vessels collect lymph from the medullary
sinus and carry it towards the venous circulation.
Lymph continues into the medullary sinus at the core of the
lymph node. This region contain B cells and plasma cells.
12](https://image.slidesharecdn.com/lnheadandneck-230217054454-2b8ac3fa/85/LN-HEAD-AND-NECK-pptx-12-320.jpg)