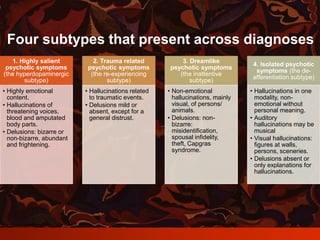
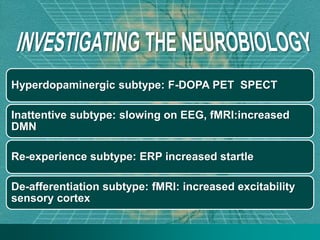
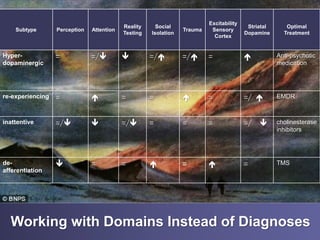
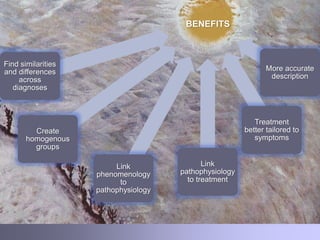
This document outlines a transdiagnostic approach to understanding psychotic symptoms across different diagnoses. It identifies four subtypes of psychotic experiences - highly salient, trauma-related, dreamlike, and isolated symptoms - that can present across conditions like schizophrenia, bipolar disorder, PTSD, and others. Each subtype is associated with different patterns in cognition, perception, and underlying neurobiology. Taking a transdiagnostic approach allows for more homogeneous patient groupings, links symptoms to pathophysiology, and ties pathophysiology to optimized treatment tailored to the specific symptom presentation rather than diagnosis alone.


















![Neuropsychiatry [2017]](https://cdn.slidesharecdn.com/ss_thumbnails/neuropsychiatricmanifestationofcommonneurologicaldisorders-171001003940-thumbnail.jpg?width=640&height=640&fit=bounds)



























































































