
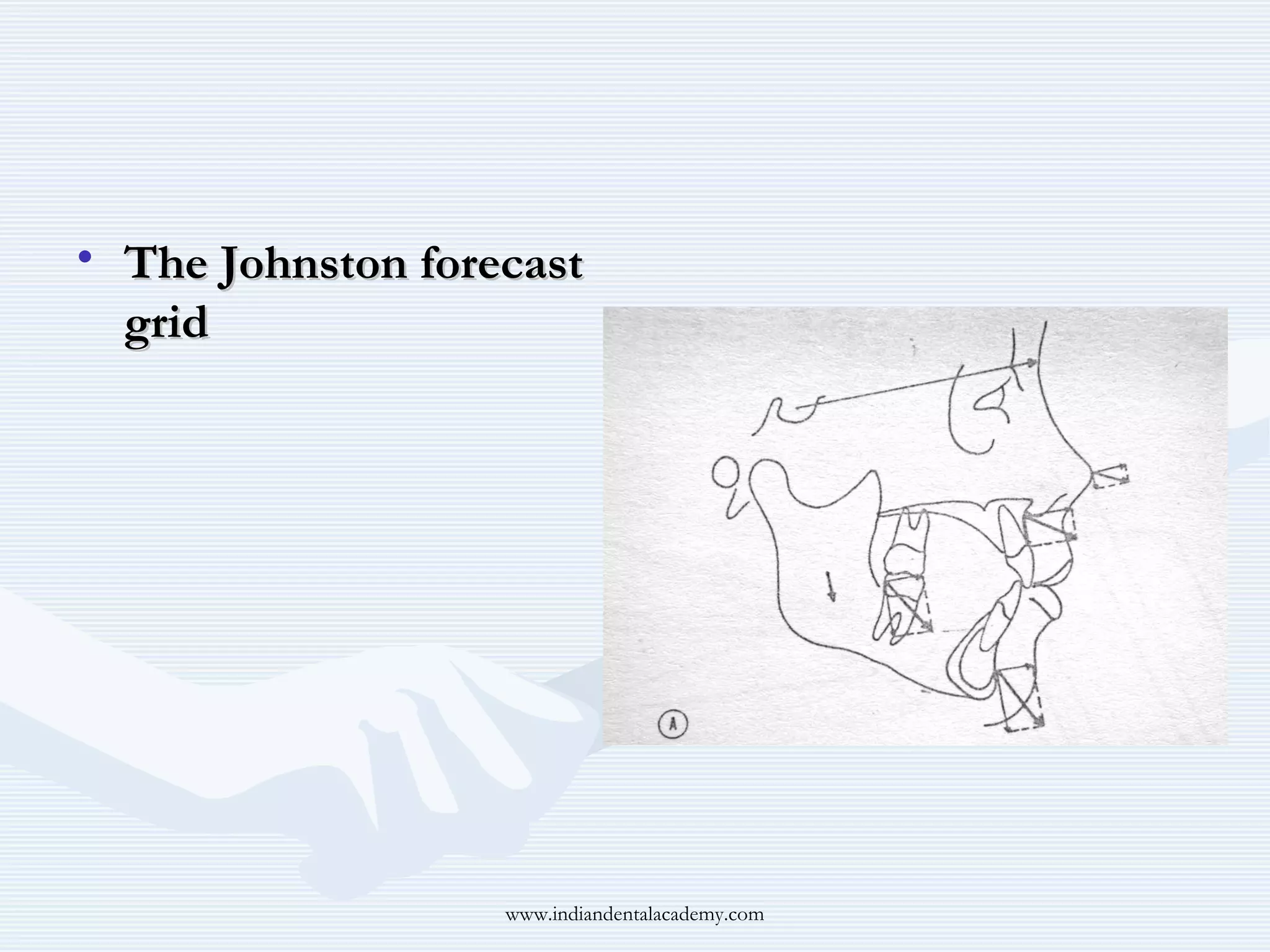

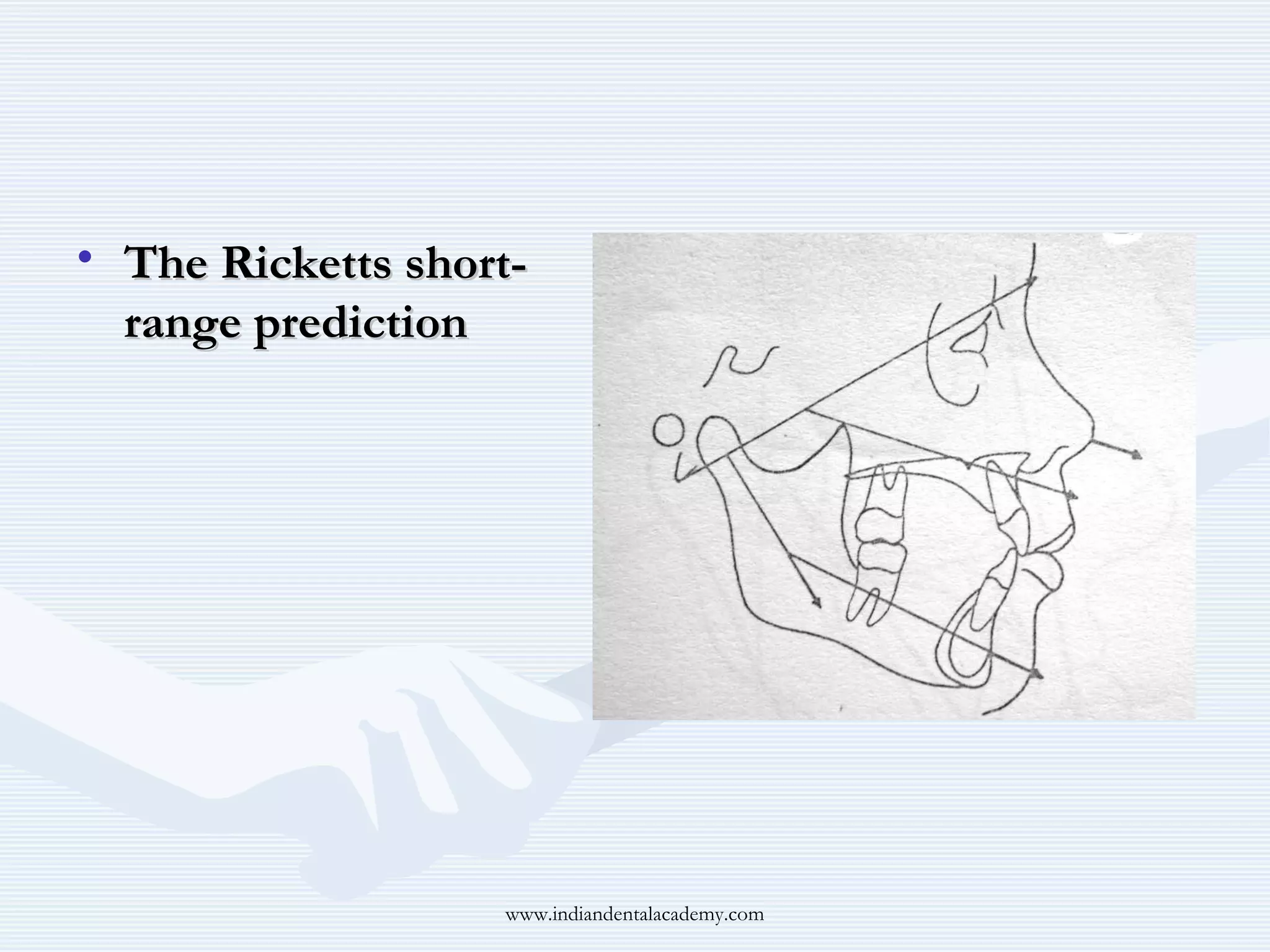

The document discusses growth predictions related to orthodontics, focusing on Holdaway's soft-tissue visual treatment objective (VTO) to create ideal facial profiles by analyzing and repositioning dental structures. It evaluates various growth forecasting methods, including Johnston's grid, Ricketts' short-range prediction, and a computer program, with the latter being the most accurate for predicting abnormal growth patterns. Additionally, a study on Ricketts' long-range prediction conducted on Turkish children reveals a higher correlation in growth predictions for girls compared to boys.





































































































