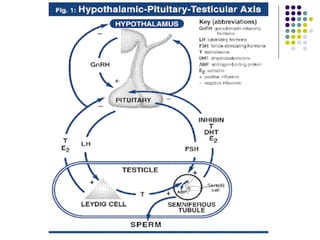
This document discusses male gonadal function and dysfunction, including causes and treatment of hypogonadism. It covers primary hypogonadism conditions like Klinefelter syndrome and secondary causes such as tumors or drugs. Diagnosis involves measuring testosterone, LH and FSH levels. Treatment options for hypogonadism include testosterone replacement therapy via patches, gels or injections, with monitoring of side effects like prostate issues.