Download as PDF, PPTX
![Table 2—Glucose-lowering medications and therapies available in the U.S. or Europe and specific characteristics that may guide individualized treatment choices in
nonpregnant adults with type 2 diabetes
Class
Medications/therapies
in class Primary physiological action(s) Advantages Disadvantages/adverse effects Efficacy
Lifestyle
Diet quality c Mediterranean type
c DASH
c Low carbohydrate
c Vegetarian
c Others
c Depends on diet c Inexpensive
c No side effects
c Requires instruction
c Requires motivation
c Requires lifelong behavioral change
c Social barriers may exist
Intermediate
Physical activity c Running, walking
c Bicycling (including
stationary)
c Swimming
c Resistance training
c Yoga
c Tai chi
c Many others
c Energy expenditure
c Weight management
c ↑ Insulin sensitivity
c Inexpensive
c ↓ Fall risk by increasing balance/strength
c ? Improves mental health
c ↑ Bone density
c ↓ Blood pressure
c ↓ Weight
c Improves ASCVD risk factors
c Risk of musculoskeletal injury
c Requires motivation
c Risk of foot trauma in patients with
neuropathy
c Requires lifelong behavioral change
Intermediate
Energy restriction c Individual energy
restriction with or
without energy tracking
c Programs with
counseling
c Food substitution
programs
c Energy restriction
c Weight management
c ↓ Hepatic and pancreatic
fat
c ↑ Insulin sensitivity
c Lowers glycemia
c Reduces need for diabetes and
other medications
c No serious side effects
c Improves ASCVD risk factors
c Requires motivation
c Requires lifelong behavioral change
Variable, with potential for
very high efficacy; often
intermediate
Oral medications
Biguanides c Metformin c ↓ Hepatic glucose production
c Multiple other non-insulin-
mediated mechanisms
c Extensive experience
c No hypoglycemia
c Inexpensive
c GI symptoms
c Vitamin B12 deficiency
c Use with caution or dose adjustment
forCKDstage3B(eGFR30–44mLmin21
[1.73 m]22
)
c Lactic acidosis (rare)
High
SGLT2 inhibitors c Canagliflozin
c Dapagliflozin
c Empagliflozin
c Ertugliflozin
c Blocks glucose reabsorption
by the kidney, increasing
glucosuria
c ? Other tubulo-glomerular
effects
c No hypoglycemia
c ↓ Weight
c ↓ Blood pressure
c Effective at all stages of T2DM
with preserved glomerular function
c ↓ MACE, HF, CKD with some
agents (see text)
c Genital infections
c UTI
c Polyuria
c Volume depletion/hypotension/
dizziness
c ↑ LDL-C
c ↑ Creatinine (transient)
c Dose adjustment/avoidance for renal
disease
c ↑ Risk for amputation (canagliflozin)
c ↑ Risk for fracture (canagliflozin)
Intermediate–high
(dependent on GFR)
Continued on p. 2682
care.diabetesjournals.orgDaviesandAssociates2681](https://image.slidesharecdn.com/diabtt-200304192948/75/Glucose-lowering-medications-1-2048.jpg)
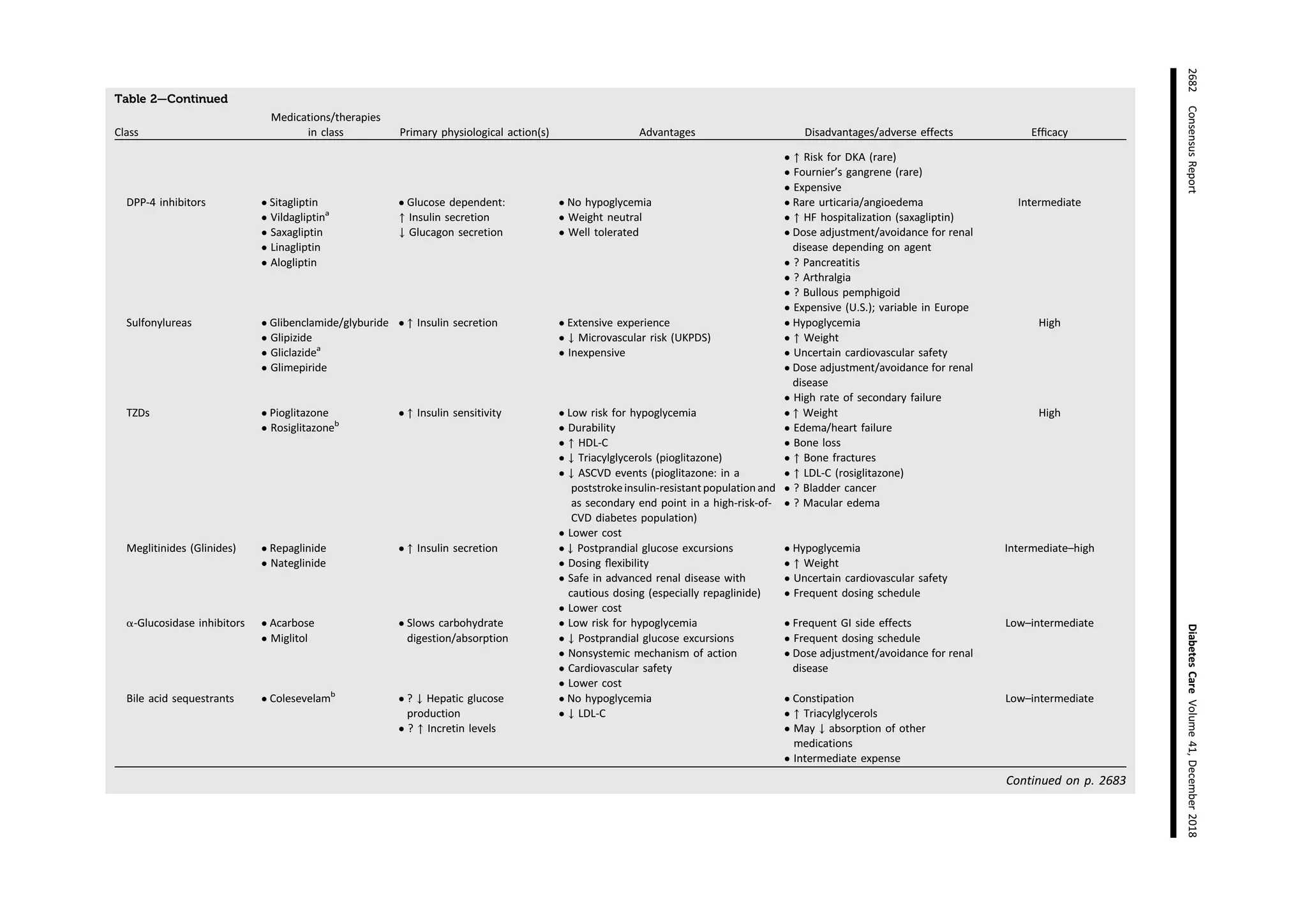




The document presents a comprehensive table detailing various glucose-lowering medications and therapies for adults with type 2 diabetes, including their physiological actions, advantages, disadvantages, and efficacy levels. It categorizes treatments into classes such as oral medications, injectable medications, and weight loss therapies, highlighting their impact on glucose control and associated risks. The information serves as a guide for individualized treatment choices based on patient needs and circumstances.



























![Anesthesia for dm-1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiafordm-11-181123085851-thumbnail.jpg?width=640&height=640&fit=bounds)























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)



