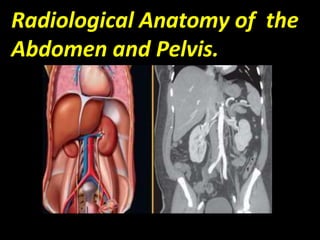
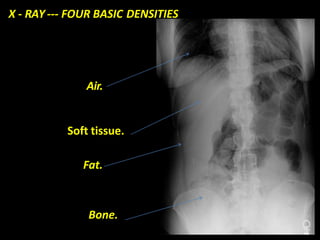
This document discusses various radiological imaging modalities used to image the abdomen and pelvis. It provides details on ultrasound, CT, MRI, plain film x-rays, fluoroscopy, and nuclear medicine scans. It describes the basic physics behind each technique and provides examples of their use. Key anatomy is reviewed along with normal expected findings and examples of common pathologies seen on plain films. A systematic approach to interpreting abdominal x-rays is also outlined.
























































![RADIOGRAPHIC_IMAGING_OF_THE_ABDOMEN[1].docx](https://cdn.slidesharecdn.com/ss_thumbnails/radiographicimagingoftheabdomen1-250705135117-4a4a689a-thumbnail.jpg?width=640&height=640&fit=bounds)