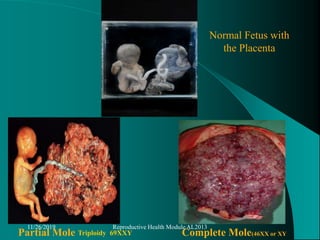
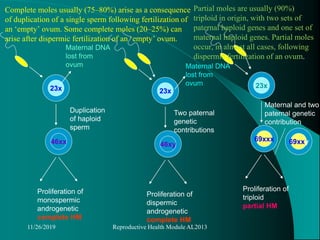
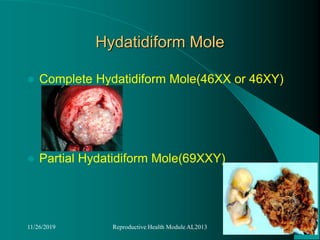
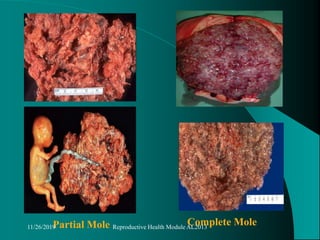
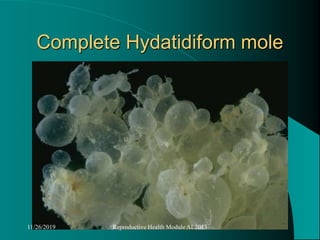
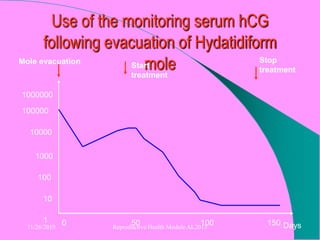
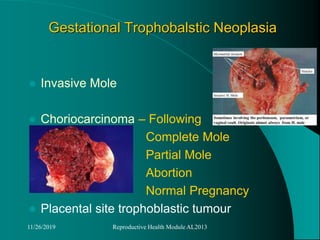
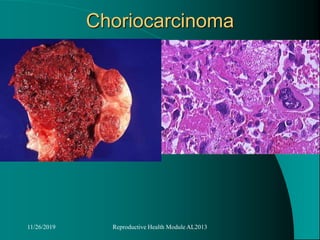
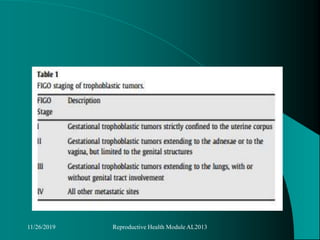
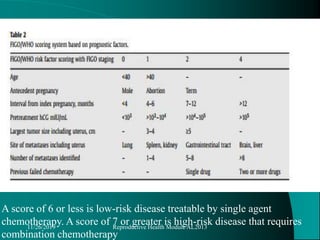
This document discusses gestational trophoblastic disease (GTD), including classifications, genetics, risk factors, clinical features, investigations, management, and follow up. GTD includes benign, non-neoplastic lesions like molar pregnancies as well as gestational trophoblastic neoplasms. Molar pregnancies are classified as complete or partial moles. Complete moles usually arise from abnormal fertilization, while partial moles are usually triploid. Follow up of molar pregnancies involves monitoring beta-hCG levels to detect persistent trophoblastic disease.