Geriatric-Related Mental Health Problems
Discuss Dementia and delirium in relation to the mental health of elderly.
Causes and Risk Factors for Mental Illness
Objectives
At the endof this session students will be able to …………..
Identify and describe the elements of a comprehensive psychiatric
assessment of elderly clients with compromised cognition
Discuss Dementia and delirium in relation to mental health of
elderly
Analyze nursing care needs for elderly clients with mental health
problems
3.
The Human LifeCycle Stages
Pre-birth
Birth
Infancy (0-3)
Early Childhood (3-6)
Middle Childhood (6-8)
Late Childhood (9-11)
Adolescence (12-20)
Early Adulthood (20-35)
Midlife (35-50)
Mature Adulthood (50-80)
Late Adulthood (80+)
Death and Dying
4.
Definition of MentalIllness
A mental illness is a condition that affects a person’s thinking,
feeling or mood. Such conditions may affect someone’s ability to
relate to others and function each day. Each person will have
different experiences, even people with the same diagnosis.
5.
Some Basics AboutGeriatrics
Changes of the brain
Changes of the body
Changes of many levels of functioning
Changes of tolerance in medication, alcohol, foods
6.
Causes and RiskFactors for Mental Illness
Physical disability
Long-term illness (e.g., heart disease, cancer)
Dementia-causing illness (e.g., Alzheimer’s disease)
Change of environment, like moving into assisted living
Illness or loss of a loved one
Medication interactions
Alcohol or substance use
Poor diet or malnutrition
7.
Symptoms of MentalIllness
Sad or depressed mood lasting longer than two weeks
Social withdrawal; loss of interest in things that used to be enjoyable
Unexplained fatigue, energy loss, or sleep changes
Confusion, disorientation, problems with concentration or decision-
making
Increase or decrease in appetite; changes in weight
Memory loss, especially recent or short-term memory problems
8.
Cont….
Feelings ofworthlessness, inappropriate guilt, helplessness; thoughts of
suicide
Physical symptoms that can’t otherwise be explained: aches,
constipation, etc.
Changes in appearance or dress, or problems maintaining the home or
yard
Trouble handling finances or working with numbers
9.
Mental Health Goals/ Interventions
Healthy adjustment to stage of life
Acceptance of loss
Involvement in life activities as fully as possible
Reminiscence therapy : to help individuals with dementia remember
events, people and places from their past lives. As part of the therapy,
care partners may use objects in various activities to help individuals
with recall of memories
10.
Cont….
Explore spirituality
Acceptance of how a person has lived their life
What are they proud about in their life
Do they want to talk about death / the after life? Do they have
an opinion about this
What is their meaning of life
11.
A Comprehensive Assessment
Thekey components of a Comprehensive Assessment include:
History
Psychosocial/developmental and personal history
Mental State
Cognitive Assessment
Substance Use
Medical/Biological – Physical assessment
Risk
12.
History
History ofpresent illness
Psychiatric history and medical history
Psychosocial/Developmental History (Personal History)
Social History
Family History
13.
Psychosocial / DevelopmentalHistory
Gather their story:
What is their current living situation?
Who are their supports?
Where did they grow up?
How would they describe their childhood?
Is their a history of trauma – what type?
Educational achievement .
14.
Social History
Currentsituation
Family
Work
Finance
Friendship groups
Hobbies - interests
15.
Family History
Genogram
Attitude to family – how do they see themselves within the
family group
Quality of relationships and contact with family
History of mental illness
History of suicide in other family members
16.
Mental State Examination
Whydo a MSE?
Provides baseline information regarding a person’s mental state at the time of
interview
Helps identify who may need a more comprehensive psychiatric assessment
To assist with diagnosis
To guide interventions
To evaluate patient’s progress
To inform the risk assessment
To support discharge planning
Structured approach to understanding the psychological state of patients
17.
When do NursesConduct MSE?
On admission – scheduled and structured and systematic data gathering
Ongoing assessment and evaluation – structures and informal
During crisis – structured and focused.
18.
Mental Status Examination
Themental state examination is
recorded under the following
headings:
Appearance and behavior
Rapport
Speech
Mood
Affect
Thought
Perception
Cognition
Insight
19.
Dementia vs. Delirium
What’s the difference, and strategies to help the patient and
caregiver
20.
Cont….
Delirium
Disturbance ofconsciousness with reduced ability to focus, sustain, or shift attention
A change in cognition, a perceptual disturbance not accounted for by preexisting,
established or evolving dementia
Occurs over a short time period and fluctuates during the day
Has a causal component
Dementia
Chronic acquired decline in memory and at least on other cognitive function
Decline usually evident over longer periods with mild to severe cognitive decline,
hallucinations, and delusions
21.
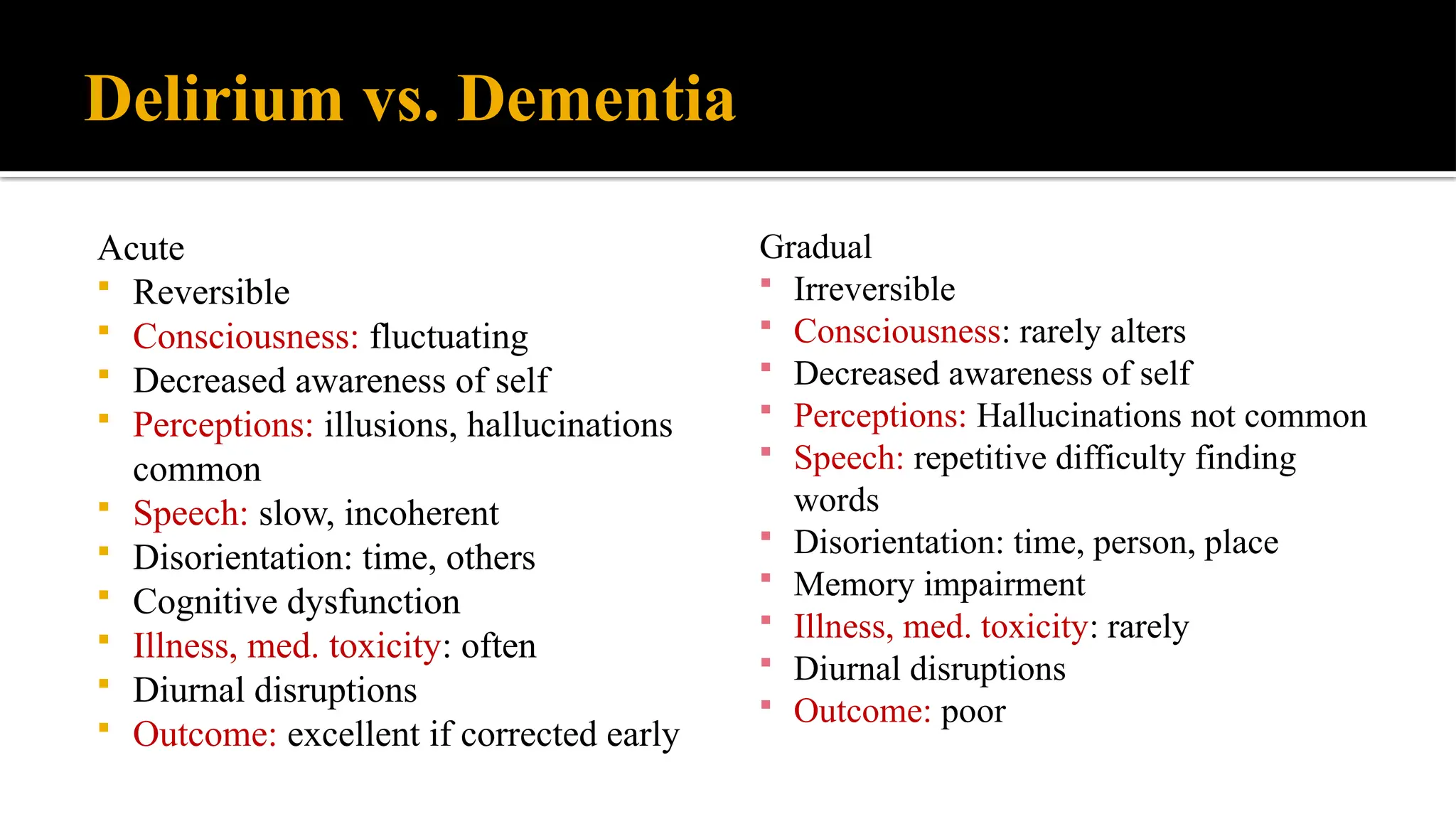
Delirium vs. Dementia
Acute
Reversible
Consciousness: fluctuating
Decreased awareness of self
Perceptions: illusions, hallucinations
common
Speech: slow, incoherent
Disorientation: time, others
Cognitive dysfunction
Illness, med. toxicity: often
Diurnal disruptions
Outcome: excellent if corrected early
Gradual
Irreversible
Consciousness: rarely alters
Decreased awareness of self
Perceptions: Hallucinations not common
Speech: repetitive difficulty finding
words
Disorientation: time, person, place
Memory impairment
Illness, med. toxicity: rarely
Diurnal disruptions
Outcome: poor
22.
Delirium
A medicalemergency
Triggered by
Oxygen deprivation
Drug use/poisons, meds
Infections, recent surgery, or trauma
Severe chronic illness
Electrolyte imbalances
Pre-morbid brain conditions, and functional status
Preexisting cognitive impairment
Old age/ sensory losses
23.
Prevention Risk factors
Cognitive impairment
Dehydration/electrolyte
imbalance
Sensory deprivation/ sleep
disturbances
Pharmacy
Routine mental status
assessment, staff education
I&O, skin assessment, early
recognition
Non pharmacologic sleep aids,
decreased noise and light at
night, frequent rest periods,
daytime activities
Staff education of medication
side effects, pharmacy link
Intervention
24.
Dementia
Comes onover time, short term memory loss becomes evident
May progress slowly or quickly
May affect younger persons as well as elderly
Treatment generally depends on the stage/ severity of the disease
Becoming old doesn’t mean you will develop dementia
25.
Nursing Management
Nursing interventionsare aimed at maintaining
Patient’s physical safety
Reducing anxiety and agitation
Promoting independence in self-care activities
Maintaining adequate nutrition
Managing sleep pattern
Supporting and educating family caregivers
Improving communication
Getting their attention
Gain the persons attention
Turn off extraneous noise
Stand in front of the person and maintain eye contact
Go slow, direct and redirect their attention
28.
Be aware ofyour tone of voice
Do not shout!
Do not speak in a condescending tone
Speak slowly
29.
Take care withyour use of language
Use adult language
Concrete simple language, short phrases
Be positive and reassuring
Don’t talk about the person as if they weren’t there
30.
Try Yes orNo Questions
Use 2 choice questions like do you want juice or soda?
Are you hungry?
Are you tired?
Can I read to you?
31.
Orient and ReorientFrequently
Use visual aids
Make sure they have hearing aids or glasses if they need them
Calendars and message boards
Keep them up to date, make sure they are easy to locate
Orient the person with your language
32.
Learn to bea Good Listener
Listen and watch/ wait for the response
Do not interrupt
Be willing to talk about old times then redirect
33.
Lastly-Don’t Argue
Theperson with dementia is not trying to be disagreeable
they are usually unaware that they are making mistakes
If the person is in immediate danger then correcting the thought or
behavior might be appropriate. If not-
DON”T ARGUE you will only cause frustration, fear and anger
34.
References
Stuart GW.Principles and Practice of Psychiatric Nursing-E-Book. Elsevier Health Sciences;
2014.
Videbeck S. Psychiatric-mental health nursing. Lippincott Williams & Wilkins; 2013 Jul 29.
Hinkle J, Cheever K, Brunner L, Suddarth D. Brunner & Suddarth's textbook of medical-
surgical nursing. Philadelphia: Wolters Kluwer Health, Lippincott Williams & Wilkins; 2014.
Thank you
Editor's Notes
#23 Keeping a regular daily routine that includes waking, dressing, meals and social activities.
#26 Communication
Is often what relationships are built on
When communication becomes faulty our relationships crumble
Our communication strategies can help an older adult with advancing dementia feel safe, less anxious, and less likely to become upset or aggressive
#27 communication can’t happen if you don’t first gain the persons attention. Turn off extraneous noise, stand in front of the person and maintain eye contact, go slow, be prepared to direct and redirect attention
#28 Do not speak in a condescending tone or in a tone you might use with a child. A person with dementia is most likely anxious and will pick up on your emotions and may become upset or angry due to misinterpretation of your intent
#29 Try to give a phrase like till the cows come home as an example of what would be not concrete
this can be extremely helpful
#30 This can make information gathering easier as the person has greater difficulty making needs known and make keep them from reacting negatively due to fear or frustration
#31 “It’s 12 noon would you like lunch.” Are you looking forward to thanksgiving, I’m so happy it’s November.
#32 Listen and watch for verbal and non-verbal cues
Listen for the intent in ramblings/ slow down the rate of conversation
Be aware of signs of frustration fatigue or overload that might lead to disruptive behavior