![Introduction International and Australasian health care organizations are seeking to improve the use of computerised clinical decision support (CDS) in health care [1;2;3] . New Zealand’s primary health care sector is now structured around not-for-profit Primary Health Organisations (PHOs) [4] . Knowledge of IT infrastructure and its usage by PHO member practices would enable their management organisations to formulate appropriate strategies to encourage better use of technologies, and the decision support capabilities they provide. This presentation gives preliminary results regarding the IT supporting patient care in primary care GP practices, and the utilisation of three of the most popular of those technologies for CDS.](https://image.slidesharecdn.com/further-evidence-of-how-technology-availability-doesnt-guarantee-usage-1195347159691343-3/85/Further-Evidence-of-How-Technology-Availability-Doesn-t-Guarantee-Usage-3-320.jpg)
![Methodology A literature review followed by a multiple case study of medium sized PHOs, consisting of a pilot case study PHO, and two other case study PHOs. Triangulation [5] was achieved by the use of face-to-face interviews, a postal questionnaire survey of GP practices and the collection of documentation at each case study organisation.](https://image.slidesharecdn.com/further-evidence-of-how-technology-availability-doesnt-guarantee-usage-1195347159691343-3/85/Further-Evidence-of-How-Technology-Availability-Doesn-t-Guarantee-Usage-6-320.jpg)
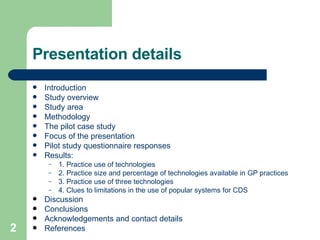
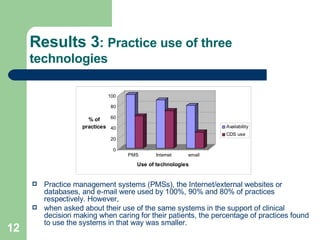
![Results 1: Practice use of technologies [a] Secure network for health sector electronic messaging Technologies used in the support of patient care by 30% or more of the respondent practices. 30 AI/expert systems (e.g. risk assessor) 80 e-mail 30 Digital camera (for mole tracking) 80 Extranet application (e.g. ACC logging) 30 Laptop 90 Spreadsheet 30 Intranet application 90 Internal messaging system 40 Remote access 90 The Internet/external websites or databases 40 Information manager (e.g. Outlook) 100 Word processing software 50 Cell-phone 100 Healthlink connection [a] 50 Scanner 100 PCs 60 Secure file transfer (e.g. Securit) 100 Printer 60 Server 100 Fax. Machine 70 Desktop publishing 100 Practice Management Systems (PMS) % Practices using technology Technology % Practices using technology Technology](https://image.slidesharecdn.com/further-evidence-of-how-technology-availability-doesnt-guarantee-usage-1195347159691343-3/85/Further-Evidence-of-How-Technology-Availability-Doesn-t-Guarantee-Usage-10-320.jpg)
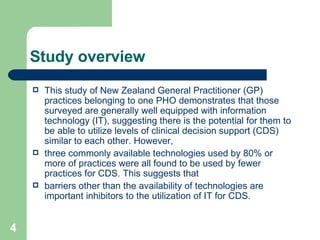
![Results 2: Practice size and percentage of technologies available in GP practices Individual practices used between 45.5% and 95.5% of the technologies shown in table 1. all but the three smallest practices [b] used more than 50% of the technologies, but otherwise there appeared to be little evidence that increasing practice size corresponded to increased technology infrastructure. [b] Practices 1-3 and are the same size, based on the total number of staff and GP FTEs in each practice](https://image.slidesharecdn.com/further-evidence-of-how-technology-availability-doesnt-guarantee-usage-1195347159691343-3/85/Further-Evidence-of-How-Technology-Availability-Doesn-t-Guarantee-Usage-11-320.jpg)
![Results 4: Clues to limitations in the use of popular systems for CDS Practice nurse’s comments: PMS and user skills - “ It’s got the capability to do that [provide alerts and reminders]. It’s only as good as the operator…We all do our own [setting up]….I use it a lot, especially for over-dues.” Access to, and use of the Internet - “ … I can gather [needed information] but I have to go outside of work to do it ... you see [the doctor’s] got the Internet for ‘travel’ which he looks up and … I have a lot of queries about travel and I have to go to him for that because I can’t directly access it myself …”](https://image.slidesharecdn.com/further-evidence-of-how-technology-availability-doesnt-guarantee-usage-1195347159691343-3/85/Further-Evidence-of-How-Technology-Availability-Doesn-t-Guarantee-Usage-13-320.jpg)
![Results 4 (cont): Clues to limitations in the use of popular systems for CDS Administrator’s comments in a practice where one of the doctors uses the Internet little and doesn’t use e-mail at all for CDS: “ Our doctors do use that [e-mail] quite a lot: for special authorities [c] - if they’ve sent one away and they haven’t got it back; for ACC [d] , if they have a lot of clients who come in and say “ACC declined my claim. What do I do now…?” We have a lot of interaction with WINZ [e] , because a lot of our clients are beneficiaries, so we have a lot to do with working with the case managers …” [c] Authorities needed for the prescription of certain subsidized medications [d] The Accident Compensation Corporation [e] Work and Income New Zealand](https://image.slidesharecdn.com/further-evidence-of-how-technology-availability-doesnt-guarantee-usage-1195347159691343-3/85/Further-Evidence-of-How-Technology-Availability-Doesn-t-Guarantee-Usage-14-320.jpg)
![Discussion cont. Such additional barriers may include resource and clinical issues such as time, cost, training, credibility, and skills in using CDS programmes, and less importantly, technical and systems considerations [6;7;8] . Actually having access to popular technologies within an organisation or even within one practice does not necessarily guarantee either their general use, or use for CDS.](https://image.slidesharecdn.com/further-evidence-of-how-technology-availability-doesnt-guarantee-usage-1195347159691343-3/85/Further-Evidence-of-How-Technology-Availability-Doesn-t-Guarantee-Usage-16-320.jpg)
![Acknowledgements and Contact Details Acknowledgements - With thanks to: the staff of the pilot case study PHO management organisation and health care practices, for their generosity in sharing their knowledge and time; the local Iwi Council of Elders, Te Mauri O Rangitaane O Manawatu for their support and advice; the Tertiary Education Commission for the support provided by a Bright Future Top Achiever Doctoral Scholarship; the Maurice and Phyllis Paykel Trust for a travel grant which contributed to the presentation of a poster based on this research which was presented at the Medinfo Congress 2007, August 20-24, Brisbane, Australia, and the Health and Disability Ethics Committee for approval for the research (reference: CEN/05/08/053). Contact details - Judith Engelbrecht, Information Systems Group, College of Business, Massey University, Palmerston North, New Zealand. Phone +64 6 356 9099 ext 7753 [email_address]](https://image.slidesharecdn.com/further-evidence-of-how-technology-availability-doesnt-guarantee-usage-1195347159691343-3/85/Further-Evidence-of-How-Technology-Availability-Doesn-t-Guarantee-Usage-18-320.jpg)
![References [1] WAVE Advisory Board. From Strategy to Reality, The WAVE Project, Kia hopu te ngaru. Wellington: Ministry of Health, 2001. [2] National Electronic Decision Support Taskforce. Electronic decision support for Australia’s health sector. National Health Information Management Advisory Council (NHIMAC). 2003 January. [Accessed 2004 October]. URL: http:// www.ahic.org.au/downloads/nedsrept.pdf [3] Metzger J and MacDonald K. Clinical decision support for the independent physician practice. First Consulting Group. California HealthCare Foundation, California: 2002 October. [Accessed 2006 November]. URL: http://www.chcf.org/documents/ihealth/ClinicalDecisionSupport.pdf [4] Ministry of Health. The primary health care strategy. Wellington: Ministry of Health, 2001. [5] Yin RK. Case Study Research: Design and Methods, 3rd ed. Applied Social Research Methods Series, vol.5. California: SAGE Publications, 2003. [6] Engelbrecht J, Whiddett R, and Hunter I. The use of information systems for clinical decision support by primary health care practices in a medium sized PHO. Health Care and Informatics Review OnlineTM. September 2006. [Accessed 2006 October]. URL: http:// hcro.enigma.co.nz/website/index.cfm?fuseaction = articledisplay&FeatureID =060906 [7] Leung GM, Yu PLH, Wong IOL, Johnston JM., and Tin KYK. Incentives and barriers that influence clinical computerization in Hong Kong: A population-based physician survey. JAMIA March/April 2003: 10: 201-212 [8] Wells S and Jackson R. Online management of cardiovascular risk in New Zealand with PREDICT™ – Getting evidence to the "moment of care". Health Care and Informatics Review OnlineTM. March 2005. [Accessed 2006 May]. URL: http:// hcro.enigma.co.nz/website/index.cfm?fuseaction = articledisplay&featureid =010305](https://image.slidesharecdn.com/further-evidence-of-how-technology-availability-doesnt-guarantee-usage-1195347159691343-3/85/Further-Evidence-of-How-Technology-Availability-Doesn-t-Guarantee-Usage-19-320.jpg)

The study investigates the use of computerized clinical decision support (CDS) technologies in New Zealand general practices, revealing that while these practices are well-equipped with technology, many are not utilizing it effectively for CDS. Barriers to usage include resource limitations, clinical issues, and a lack of training rather than the technology's availability. To enhance CDS usage, primary health care managers need to understand the specific IT infrastructure and barriers to the technology's application in their practices.






















































































