FRACTURE OF SCAPULA:ZDARKOVIC AND DAMHOLT
(BASED ON ANATOMICAL LOCATION)
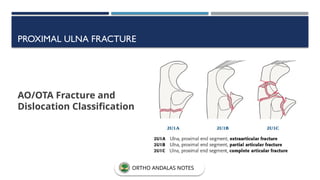
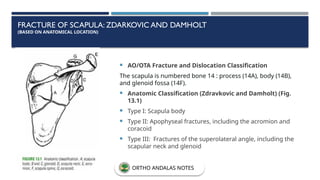
AO/OTA Fracture and Dislocation Classification
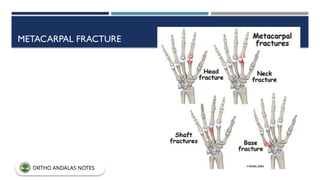
The scapula is numbered bone 14 : process (14A), body (14B),
and glenoid fossa (14F).
Anatomic Classification (Zdravkovic and Damholt) (Fig.
13.1)
Type I: Scapula body
Type II: Apophyseal fractures, including the acromion and
coracoid
Type III: Fractures of the superolateral angle, including the
scapular neck and glenoid
ORTHO ANDALAS NOTES
6.
IDEBERG CLASSIFICATION
(BASED ONDISPLACEMENT OF THE ARTICULAR COMPONENT)
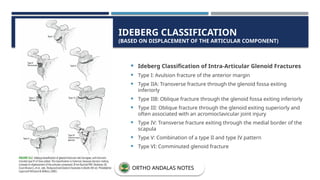
Ideberg Classification of Intra-Articular Glenoid Fractures
Type I: Avulsion fracture of the anterior margin
Type IIA: Transverse fracture through the glenoid fossa exiting
inferiorly
Type IIB: Oblique fracture through the glenoid fossa exiting inferiorly
Type III: Oblique fracture through the glenoid exiting superiorly and
often associated with an acromioclavicular joint injury
Type IV: Transverse fracture exiting through the medial border of the
scapula
Type V: Combination of a type II and type IV pattern
Type VI: Comminuted glenoid fracture
ORTHO ANDALAS NOTES
7.
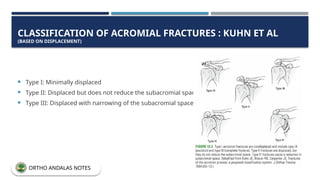
CLASSIFICATION OF ACROMIALFRACTURES : KUHN ET AL
(BASED ON DISPLACEMENT)
Type I: Minimally displaced
Type II: Displaced but does not reduce the subacromial space
Type III: Displaced with narrowing of the subacromial space
ORTHO ANDALAS NOTES
8.
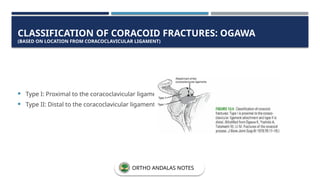
CLASSIFICATION OF CORACOIDFRACTURES: OGAWA
(BASED ON LOCATION FROM CORACOCLAVICULAR LIGAMENT)
Type I: Proximal to the coracoclavicular ligament
Type II: Distal to the coracoclavicular ligament
ORTHO ANDALAS NOTES
9.
CLAVICLE FRACTURE
AO/OTA Fractureand Dislocation Classification
15.1 (proximal [medial]), 15.2 (diaphyseal), and 15.3 (distal [lateral]).
The proximal (medial) and distal (lateral) end segments are divided into types A (extraarticular), B
(partial articular), and C (complete articular).
The diaphyseal seg-ment is divided into types A (simple), B (wedge), and C (multifragmentary)
ORTHO ANDALAS NOTES
10.
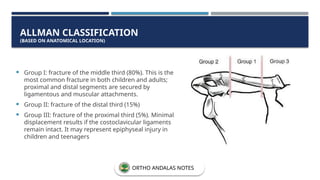
Group I:fracture of the middle third (80%). This is the
most common fracture in both children and adults;
proximal and distal segments are secured by
ligamentous and muscular attachments.
Group II: fracture of the distal third (15%)
Group III: fracture of the proximal third (5%). Minimal
displacement results if the costoclavicular ligaments
remain intact. It may represent epiphyseal injury in
children and teenagers
ALLMAN CLASSIFICATION
(BASED ON ANATOMICAL LOCATION)
ORTHO ANDALAS NOTES
11.
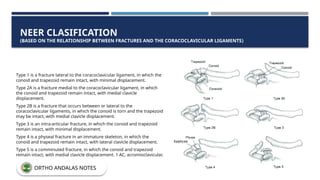
Type 1 isa fracture lateral to the coracoclavicular ligament, in which the
conoid and trapezoid remain intact, with minimal displacement.
Type 2A is a fracture medial to the coracoclavicular ligament, in which
the conoid and trapezoid remain intact, with medial clavicle
displacement.
Type 2B is a fracture that occurs between or lateral to the
coracoclavicular ligaments, in which the conoid is torn and the trapezoid
may be intact, with medial clavicle displacement.
Type 3 is an intra-articular fracture, in which the conoid and trapezoid
remain intact, with minimal displacement.
Type 4 is a physeal fracture in an immature skeleton, in which the
conoid and trapezoid remain intact, with lateral clavicle displacement.
Type 5 is a comminuted fracture, in which the conoid and trapezoid
remain intact, with medial clavicle displacement. 1 AC, acromioclavicular.
NEER CLASIFICATION
(BASED ON THE RELATIONSHIP BETWEEN FRACTURES AND THE CORACOCLAVICULAR LIGAMENTS)
ORTHO ANDALAS NOTES
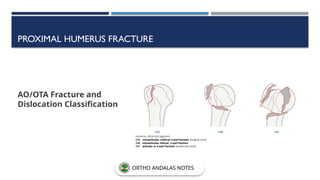
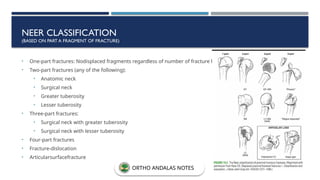
• One-part fractures:Nodisplaced fragments regardless of number of fracture lines
• Two-part fractures (any of the following):
• Anatomic neck
• Surgical neck
• Greater tuberosity
• Lesser tuberosity
• Three-part fractures:
• Surgical neck with greater tuberosity
• Surgical neck with lesser tuberosity
• Four-part fractures
• Fracture-dislocation
• Articularsurfacefracture
NEER CLASSIFICATION
(BASED ON PART A FRAGMENT OF FRACTURE)
ORTHO ANDALAS NOTES
16.
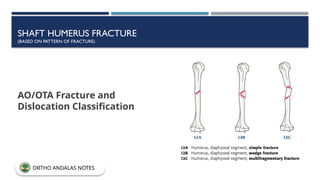
SHAFT HUMERUS FRACTURE
(BASEDON PATTERN OF FRACTURE)
AO/OTA Fracture and
Dislocation Classification
ORTHO ANDALAS NOTES
17.
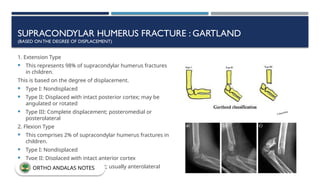
SUPRACONDYLAR HUMERUS FRACTURE: GARTLAND
(BASED ONTHE DEGREE OF DISPLACEMENT)
1. Extension Type
This represents 98% of supracondylar humerus fractures
in children.
This is based on the degree of displacement.
Type I: Nondisplaced
Type II: Displaced with intact posterior cortex; may be
angulated or rotated
Type III: Complete displacement; posteromedial or
posterolateral
2. Flexion Type
This comprises 2% of supracondylar humerus fractures in
children.
Type I: Nondisplaced
Type II: Displaced with intact anterior cortex
Type III: Complete displacement; usually anterolateral
ORTHO ANDALAS NOTES
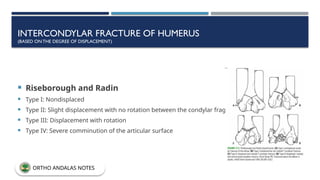
INTERCONDYLAR FRACTURE OFHUMERUS
(BASED ONTHE DEGREE OF DISPLACEMENT)
Riseborough and Radin
Type I: Nondisplaced
Type II: Slight displacement with no rotation between the condylar fragments
Type III: Displacement with rotation
Type IV: Severe comminution of the articular surface
ORTHO ANDALAS NOTES
20.
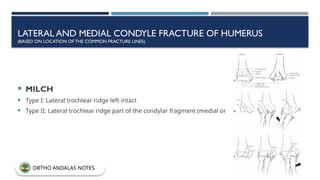
LATERAL AND MEDIALCONDYLE FRACTURE OF HUMERUS
(BASED ON LOCATION OF THE COMMON FRACTURE LINES)
MILCH
Type I: Lateral trochlear ridge left intact
Type II: Lateral trochlear ridge part of the condylar fragment (medial or lateral)
ORTHO ANDALAS NOTES
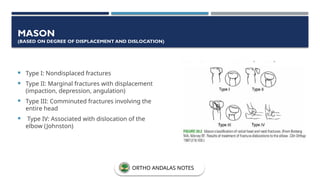
MASON
(BASED ON DEGREEOF DISPLACEMENT AND DISLOCATION)
Type I: Nondisplaced fractures
Type II: Marginal fractures with displacement
(impaction, depression, angulation)
Type III: Comminuted fractures involving the
entire head
Type IV: Associated with dislocation of the
elbow (Johnston)
ORTHO ANDALAS NOTES
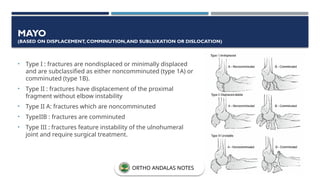
MAYO
(BASED ON DISPLACEMENT,COMMINUTION,AND SUBLUXATION OR DISLOCATION)
• Type I : fractures are nondisplaced or minimally displaced
and are subclassified as either noncomminuted (type 1A) or
comminuted (type 1B).
• Type II : fractures have displacement of the proximal
fragment without elbow instability
• Type II A: fractures which are noncomminuted
• TypeIIB : fractures are comminuted
• Type III : fractures feature instability of the ulnohumeral
joint and require surgical treatment.
ORTHO ANDALAS NOTES
25.
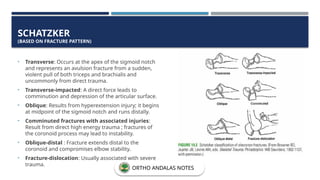
SCHATZKER
(BASED ON FRACTUREPATTERN)
• Transverse: Occurs at the apex of the sigmoid notch
and represents an avulsion fracture from a sudden,
violent pull of both triceps and brachialis and
uncommonly from direct trauma.
• Transverse-impacted: A direct force leads to
comminution and depression of the articular surface.
• Oblique: Results from hyperextension injury; it begins
at midpoint of the sigmoid notch and runs distally.
• Comminuted fractures with associated injuries:
Result from direct high energy trauma ; fractures of
the coronoid process may lead to instability.
• Oblique-distal : Fracture extends distal to the
coronoid and compromises elbow stability.
• Fracture-dislocation: Usually associated with severe
trauma.
ORTHO ANDALAS NOTES
26.
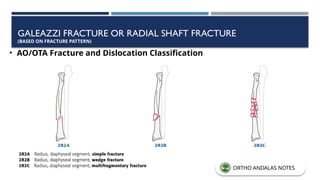
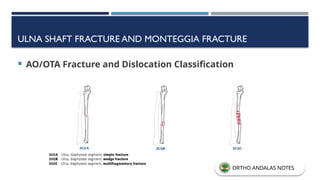
GALEAZZI FRACTURE ORRADIAL SHAFT FRACTURE
(BASED ON FRACTURE PATTERN)
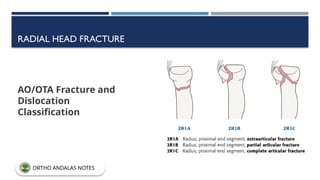
• AO/OTA Fracture and Dislocation Classification
ORTHO ANDALAS NOTES
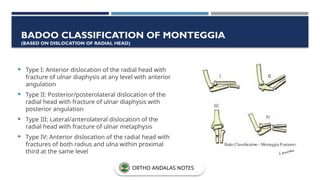
Type I:Anterior dislocation of the radial head with
fracture of ulnar diaphysis at any level with anterior
angulation
Type II: Posterior/posterolateral dislocation of the
radial head with fracture of ulnar diaphysis with
posterior angulation
Type III: Lateral/anterolateral dislocation of the
radial head with fracture of ulnar metaphysis
Type IV: Anterior dislocation of the radial head with
fractures of both radius and ulna within proximal
third at the same level
BADOO CLASSIFICATION OF MONTEGGIA
(BASED ON DISLOCATION OF RADIAL HEAD)
ORTHO ANDALAS NOTES
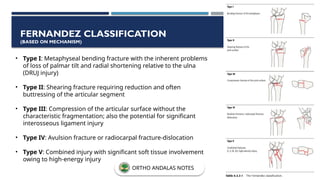
• Type I:Metaphyseal bending fracture with the inherent problems
of loss of palmar tilt and radial shortening relative to the ulna
(DRUJ injury)
• Type II: Shearing fracture requiring reduction and often
buttressing of the articular segment
• Type III: Compression of the articular surface without the
characteristic fragmentation; also the potential for significant
interosseous ligament injury
• Type IV: Avulsion fracture or radiocarpal fracture-dislocation
• Type V: Combined injury with significant soft tissue involvement
owing to high-energy injury
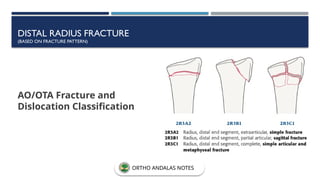
FERNANDEZ CLASSIFICATION
(BASED ON MECHANISM)
ORTHO ANDALAS NOTES
SCAPHOID FRACTURE
(BASED ONLOCATION OF FRACTURE LINE)
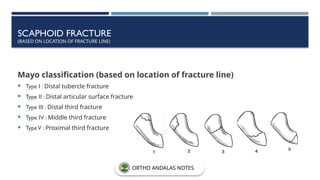
Mayo classification (based on location of fracture line)
Type I : Distal tubercle fracture
Type II : Distal articular surface fracture
Type III : Distal third fracture
Type IV : Middle third fracture
TypeV : Proximal third fracture
ORTHO ANDALAS NOTES
OCCIPITAL CONDYLE FRACTURES
Type I: Impaction of
condyle; usually stable
Type II: Shear injury
associated with basilar
or skull fractures;
potentially unstable
Type III: Condylar
avulsion; unstable
ORTHO ANDALAS NOTES
40.
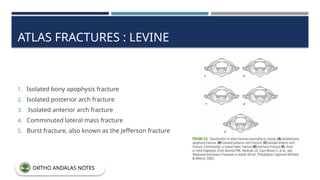
ATLAS FRACTURES :LEVINE
1. Isolated bony apophysis fracture
2. Isolated posterior arch fracture
3. Isolated anterior arch fracture
4. Comminuted lateral mass fracture
5. Burst fracture, also known as the Jefferson fracture
ORTHO ANDALAS NOTES
41.
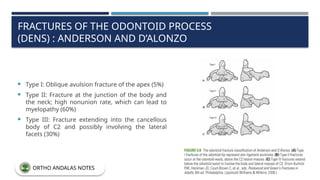
FRACTURES OF THEODONTOID PROCESS
(DENS) : ANDERSON AND D’ALONZO
Type I: Oblique avulsion fracture of the apex (5%)
Type II: Fracture at the junction of the body and
the neck; high nonunion rate, which can lead to
myelopathy (60%)
Type III: Fracture extending into the cancellous
body of C2 and possibly involving the lateral
facets (30%)
ORTHO ANDALAS NOTES
42.
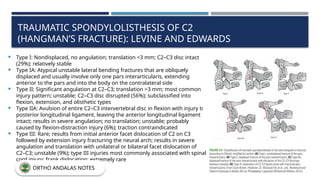
TRAUMATIC SPONDYLOLISTHESIS OFC2
(HANGMAN’S FRACTURE): LEVINE AND EDWARDS
Type I: Nondisplaced, no angulation; translation <3 mm; C2–C3 disc intact
(29%); relatively stable
Type IA: Atypical unstable lateral bending fractures that are obliquely
displaced and usually involve only one pars interarticularis, extending
anterior to the pars and into the body on the contralateral side
Type II: Significant angulation at C2–C3; translation >3 mm; most common
injury pattern; unstable; C2–C3 disc disrupted (56%); subclassified into
flexion, extension, and olisthetic types
Type IIA: Avulsion of entire C2–C3 intervertebral disc in flexion with injury to
posterior longitudinal ligament, leaving the anterior longitudinal ligament
intact; results in severe angulation; no translation; unstable; probably
caused by flexion-distraction injury (6%); traction contraindicated
Type III: Rare; results from initial anterior facet dislocation of C2 on C3
followed by extension injury fracturing the neural arch; results in severe
angulation and translation with unilateral or bilateral facet dislocation of
C2–C3; unstable (9%); type III injuries most commonly associated with spinal
cord injury; frank dislocation; extremely rare
ORTHO ANDALAS NOTES
43.
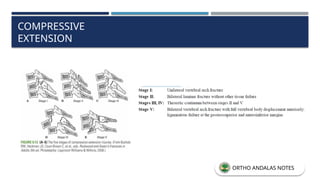
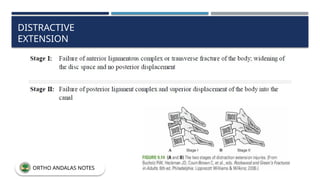
INJURIES TO C3–C7
CLASSIFICATION(ALLEN-FERGUSON)
COMPRESSIVE FLEXION (SHEAR MECHANISM RESULTING IN “TEARDROP” FRACTURES)
ORTHO ANDALAS NOTES
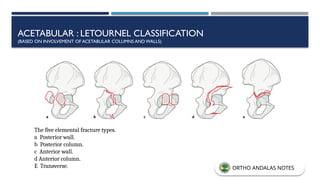
ACETABULAR : LETOURNELCLASSIFICATION
(BASED ON INVOLVEMENT OF ACETABULAR COLUMNS AND WALLS)
The five elemental fracture types.
a Posterior wall.
b Posterior column.
c Anterior wall.
d Anterior column.
E Transverse. ORTHO ANDALAS NOTES
61.
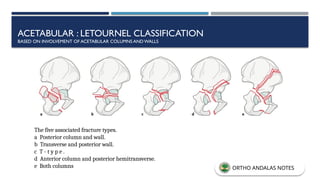
ACETABULAR : LETOURNELCLASSIFICATION
BASED ON INVOLVEMENT OF ACETABULAR COLUMNS ANDWALLS
The five associated fracture types.
a Posterior column and wall.
b Transverse and posterior wall.
c T - t y p e .
d Anterior column and posterior hemitransverse.
e Both columns ORTHO ANDALAS NOTES
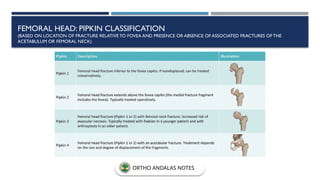
FEMORAL HEAD: PIPKINCLASSIFICATION
(BASED ON LOCATION OF FRACTURE RELATIVE TO FOVEA AND PRESENCE OR ABSENCE OF ASSOCIATED FRACTURES OF THE
ACETABULUM OR FEMORAL NECK)
ORTHO ANDALAS NOTES
64.
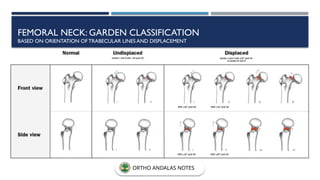
FEMORAL NECK: GARDENCLASSIFICATION
BASED ON ORIENTATION OFTRABECULAR LINES AND DISPLACEMENT
ORTHO ANDALAS NOTES
65.
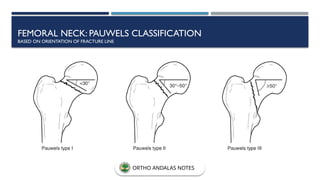
FEMORAL NECK: PAUWELSCLASSIFICATION
BASED ON ORIENTATION OF FRACTURE LINE
ORTHO ANDALAS NOTES
66.
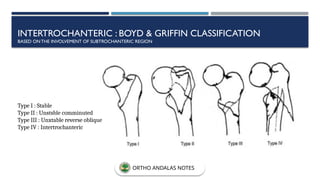
INTERTROCHANTERIC : BOYD& GRIFFIN CLASSIFICATION
BASED ONTHE INVOLVEMENT OF SUBTROCHANTERIC REGION
Type I : Stable
Type II : Unstsble comminuted
Type III : Unxtable reverse oblique
Type IV : Intertrochanteric
ORTHO ANDALAS NOTES
67.
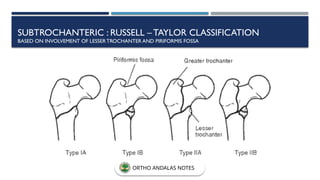
SUBTROCHANTERIC : RUSSELL–TAYLOR CLASSIFICATION
BASED ON INVOLVEMENT OF LESSERTROCHANTER AND PIRIFORMIS FOSSA
ORTHO ANDALAS NOTES
68.
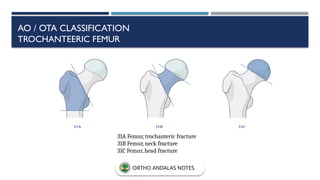
AO / OTACLASSIFICATION
TROCHANTEERIC FEMUR
31A Femur, trochanteric fracture
31B Femur, neck fracture
31C Femur, head fracture
ORTHO ANDALAS NOTES
69.
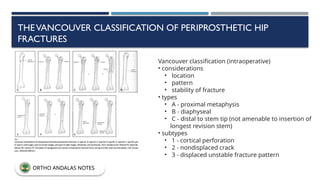
THEVANCOUVER CLASSIFICATION OFPERIPROSTHETIC HIP
FRACTURES
Vancouver classification (intraoperative)
• considerations
• location
• pattern
• stability of fracture
• types
• A - proximal metaphysis
• B - diaphyseal
• C - distal to stem tip (not amenable to insertion of
longest revision stem)
• subtypes
• 1 - cortical perforation
• 2 - nondisplaced crack
• 3 - displaced unstable fracture pattern
ORTHO ANDALAS NOTES
70.
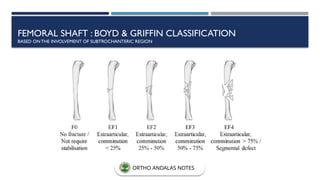
FEMORAL SHAFT :BOYD & GRIFFIN CLASSIFICATION
BASED ONTHE INVOLVEMENT OF SUBTROCHANTERIC REGION
ORTHO ANDALAS NOTES
71.
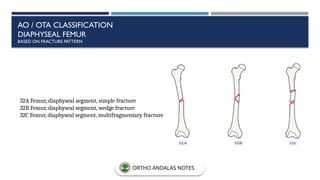
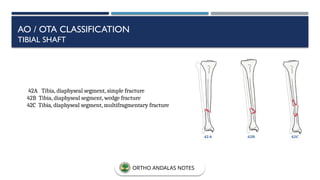
AO / OTACLASSIFICATION
DIAPHYSEAL FEMUR
BASED ON FRACTURE PATTERN
32A Femur, diaphyseal segment, simple fracture
32B Femur, diaphyseal segment, wedge fracture
32C Femur, diaphyseal segment, multifragmentary fracture
ORTHO ANDALAS NOTES
72.
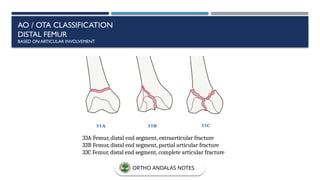
AO / OTACLASSIFICATION
DISTAL FEMUR
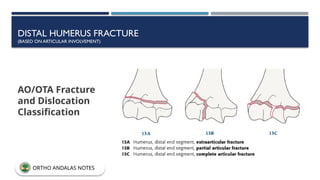
BASED ON ARTICULAR INVOLVEMENT
33A Femur, distal end segment, extraarticular fracture
33B Femur, distal end segment, partial articular fracture
33C Femur, distal end segment, complete articular fracture
ORTHO ANDALAS NOTES
73.
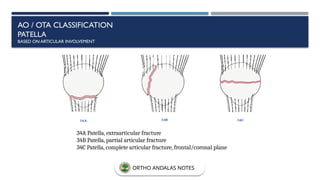
AO / OTACLASSIFICATION
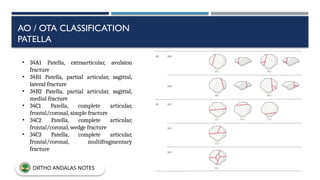
PATELLA
BASED ON ARTICULAR INVOLVEMENT
34A Patella, extraarticular fracture
34B Patella, partial articular fracture
34C Patella, complete articular fracture, frontal/coronal plane
ORTHO ANDALAS NOTES
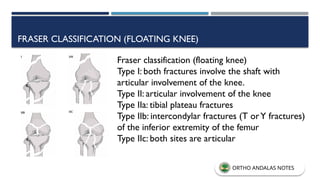
FRASER CLASSIFICATION (FLOATINGKNEE)
Fraser classification (floating knee)
Type I: both fractures involve the shaft with
articular involvement of the knee.
Type II: articular involvement of the knee
Type IIa: tibial plateau fractures
Type IIb: intercondylar fractures (T orY fractures)
of the inferior extremity of the femur
Type IIc: both sites are articular
ORTHO ANDALAS NOTES
76.
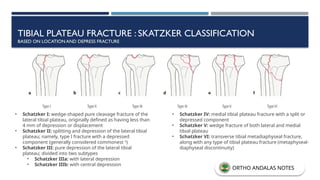
TIBIAL PLATEAU FRACTURE: SKATZKER CLASSIFICATION
BASED ON LOCATION AND DEPRESS FRACTURE
• Schatzker I: wedge-shaped pure cleavage fracture of the
lateral tibial plateau, originally defined as having less than
4 mm of depression or displacement
• Schatzker II: splitting and depression of the lateral tibial
plateau; namely, type I fracture with a depressed
component (generally considered commonest 5
)
• Schatzker III: pure depression of the lateral tibial
plateau; divided into two subtypes
• Schatzker IIIa: with lateral depression
• Schatzker IIIb: with central depression
• Schatzker IV: medial tibial plateau fracture with a split or
depressed component
• Schatzker V: wedge fracture of both lateral and medial
tibial plateau
• Schatzker VI: transverse tibial metadiaphyseal fracture,
along with any type of tibial plateau fracture (metaphyseal-
diaphyseal discontinuity)
ORTHO ANDALAS NOTES
77.
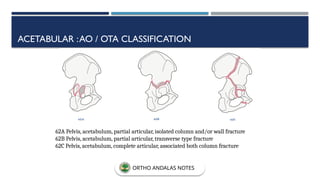
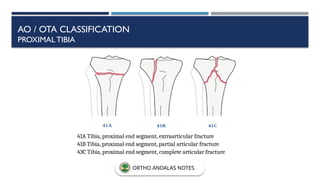
AO / OTACLASSIFICATION
PROXIMAL TIBIA
41A Tibia, proximal end segment, extraarticular fracture
41B Tibia, proximal end segment, partial articular fracture
43C Tibia, proximal end segment, complete articular fracture
ORTHO ANDALAS NOTES
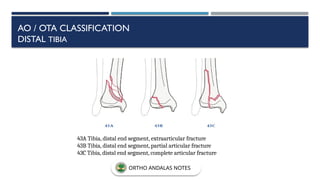
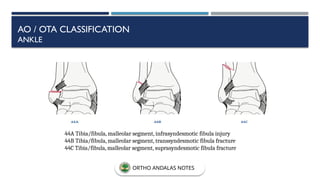
43A Tibia, distalend segment, extraarticular fracture
43B Tibia, distal end segment, partial articular fracture
43C Tibia, distal end segment, complete articular fracture
AO / OTA CLASSIFICATION
DISTAL TIBIA
ORTHO ANDALAS NOTES
80.
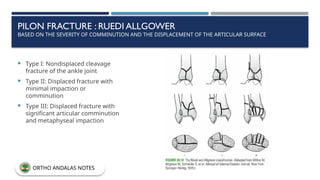
PILON FRACTURE :RUEDI ALLGOWER
BASED ON THE SEVERITY OF COMMINUTION AND THE DISPLACEMENT OF THE ARTICULAR SURFACE
Type I: Nondisplaced cleavage
fracture of the ankle joint
Type II: Displaced fracture with
minimal impaction or
comminution
Type III: Displaced fracture with
significant articular comminution
and metaphyseal impaction
ORTHO ANDALAS NOTES
ROTATIONAL ANKLE FRACTURE: LAUGE HANSEN
BASED ON “PURE” INJURY SEQUENCES, EACH SUBDIVIDED INTO STAGES OF INCREASING SEVERITY
• This system is based on cadaveric studies.
• Patterns may not always reflect clinical reality
• The system takes into account (1) the position of the foot at the time of injury and (2)
the direction
• of the deforming force.
ORTHO ANDALAS NOTES
83.
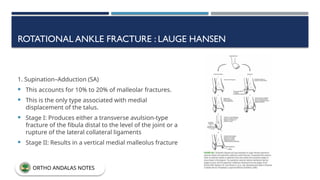
ROTATIONAL ANKLE FRACTURE: LAUGE HANSEN
1. Supination–Adduction (SA)
This accounts for 10% to 20% of malleolar fractures.
This is the only type associated with medial
displacement of the talus.
Stage I: Produces either a transverse avulsion-type
fracture of the fibula distal to the level of the joint or a
rupture of the lateral collateral ligaments
Stage II: Results in a vertical medial malleolus fracture
ORTHO ANDALAS NOTES
84.
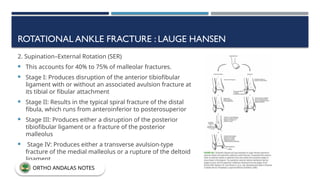
ROTATIONAL ANKLE FRACTURE: LAUGE HANSEN
2. Supination–External Rotation (SER)
This accounts for 40% to 75% of malleolar fractures.
Stage I: Produces disruption of the anterior tibiofibular
ligament with or without an associated avulsion fracture at
its tibial or fibular attachment
Stage II: Results in the typical spiral fracture of the distal
fibula, which runs from anteroinferior to posterosuperior
Stage III: Produces either a disruption of the posterior
tibiofibular ligament or a fracture of the posterior
malleolus
Stage IV: Produces either a transverse avulsion-type
fracture of the medial malleolus or a rupture of the deltoid
ligament
ORTHO ANDALAS NOTES
85.
ROTATIONAL ANKLE FRACTURE: LAUGE HANSEN
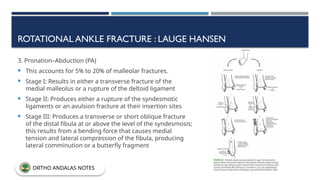
3. Pronation–Abduction (PA)
This accounts for 5% to 20% of malleolar fractures.
Stage I: Results in either a transverse fracture of the
medial malleolus or a rupture of the deltoid ligament
Stage II: Produces either a rupture of the syndesmotic
ligaments or an avulsion fracture at their insertion sites
Stage III: Produces a transverse or short oblique fracture
of the distal fibula at or above the level of the syndesmosis;
this results from a bending force that causes medial
tension and lateral compression of the fibula, producing
lateral comminution or a butterfly fragment
ORTHO ANDALAS NOTES
86.
ROTATIONAL ANKLE FRACTURE: LAUGE HANSEN
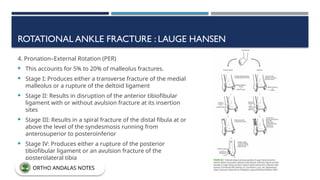
4. Pronation–External Rotation (PER)
This accounts for 5% to 20% of malleolus fractures.
Stage I: Produces either a transverse fracture of the medial
malleolus or a rupture of the deltoid ligament
Stage II: Results in disruption of the anterior tibiofibular
ligament with or without avulsion fracture at its insertion
sites
Stage III: Results in a spiral fracture of the distal fibula at or
above the level of the syndesmosis running from
anterosuperior to posteroinferior
Stage IV: Produces either a rupture of the posterior
tibiofibular ligament or an avulsion fracture of the
posterolateral tibia
ORTHO ANDALAS NOTES
87.
ROTATIONAL ANKLE FRACTURE: LAUGE HANSEN
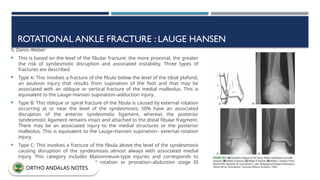
5. Danis–Weber
This is based on the level of the fibular fracture: the more proximal, the greater
the risk of syndesmotic disruption and associated instability. Three types of
fractures are described
Type A: This involves a fracture of the fibula below the level of the tibial plafond,
an avulsion injury that results from supination of the foot and that may be
associated with an oblique or vertical fracture of the medial malleolus. This is
equivalent to the Lauge–Hansen supination–adduction injury.
Type B: This oblique or spiral fracture of the fibula is caused by external rotation
occurring at or near the level of the syndesmosis; 50% have an associated
disruption of the anterior syndesmotic ligament, whereas the posterior
syndesmotic ligament remains intact and attached to the distal fibular fragment.
There may be an associated injury to the medial structures or the posterior
malleolus. This is equivalent to the Lauge–Hansen supination– external rotation
injury.
Type C: This involves a fracture of the fibula above the level of the syndesmosis
causing disruption of the syndesmosis almost always with associated medial
injury. This category includes Maisonneuve-type injuries and corresponds to
Lauge–Hansen pronation–external rotation or pronation–abduction stage III
injuries.
ORTHO ANDALAS NOTES
88.
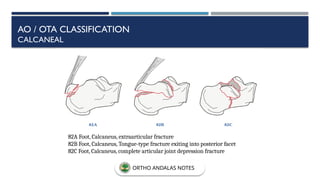
82A Foot, Calcaneus,extraarticular fracture
82B Foot, Calcaneus, Tongue-type fracture exiting into posterior facet
82C Foot, Calcaneus, complete articular joint depression fracture
AO / OTA CLASSIFICATION
CALCANEAL
ORTHO ANDALAS NOTES
89.
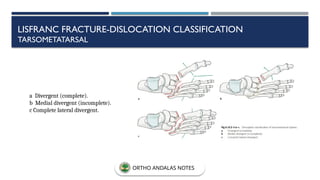
a Divergent (complete).
bMedial divergent (incomplete).
c Complete lateral divergent.
LISFRANC FRACTURE-DISLOCATION CLASSIFICATION
TARSOMETATARSAL
ORTHO ANDALAS NOTES
![CLAVICLE FRACTURE
AO/OTA Fracture and Dislocation Classification
15.1 (proximal [medial]), 15.2 (diaphyseal), and 15.3 (distal [lateral]).
The proximal (medial) and distal (lateral) end segments are divided into types A (extraarticular), B
(partial articular), and C (complete articular).
The diaphyseal seg-ment is divided into types A (simple), B (wedge), and C (multifragmentary)
ORTHO ANDALAS NOTES](https://image.slidesharecdn.com/fractureclassifications-250828044501-97e4eac8/85/FRACTURE-CLAsfdfghdghgfhghSSIFICATIONS-pptx-9-320.jpg)