Anatomy and Embryologydepartment
Fetal Membranes
ALAZHAR UNIVERSITY
Faculty of Medicine for Girls
Year 1-Semester 1
Academic year: 2022 / 2023
Module Name: Normal Human Body
Course code: IMP 07- 10103
Credit hours: 7 crh
3.
Fetal Membranes
Definition:
The fetalmembranes include all those structures that develop
from the zygot, but not share in the formation of the embryo.
These include :the placenta and umbilical cord which are not
actually membranes.
The true fetal membranes are:
(1)Chorine. (2) Amnion. (3) Yolk sac.
(4) Connecting stalk. (5) Allanto-enteric diverticulum.
Definition:
The chorion isthe wall of the chorionic vesicle.
it is formed of three layers:
1- Syncytio-trophoblast. 2- Cytotrophoblast.
3- Outer layers of primary mesoderm.
Development of chroion:
Before implantion, the outer wall of blastocyst is called trophoblast.
When implantation starts, the trophoblast is differentiated into two layers:
1- Outer syncytio-trophoblast (Cytoplasm containing many scattered nuclei.
2- Inner cytotrophoblast: which definite cell boundaries.
3- Cell from the cyto-trophoblast delaminates to form a very loose tissue
called primary (extra-embryonic mesoderm).
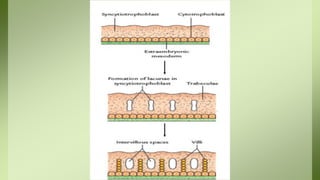
7.
Development of chorionicvilli:
The syncytio-trophoblast invades the uterine mucosa,
erode its tissue and the wall of blood vessels of
endometrium (decidua)
The syncytio-trophoblast forms irregular projections
(chronic villi).
The villi are separated by lacunae filled with maternal
blood derived from the blood vessels in the decidua. These
lacunae are the future intervillous spaces
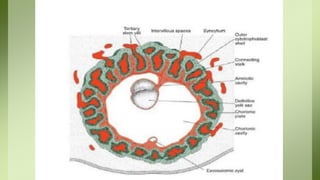
9.
Stages of developmentof chorionic villi :
1) Primary chorionic villi:
it is formed of (a) Central core of cyto-trophoblast.
(b) Covered by a layer of syncytio-trophoblast.
2) Secondary chorionic villi:
it is consisted of: (a) Central core of extra-embryonic mesoderm.
(b) The mesodermal core is surrounded by a layer of cyto-
trophoblast.
(c) The cyto-trophoblast is surrounded by a layer of syncytio-
trophoblast.
10.
3)Tertiary chorionic villi:
Themesodermal cells in the core of villus differentiated
into blood cells and small blood vessels, forming villus
capillary system.
The capillaries in the tertiary villi make contact with the
capillaries developing in the mesoderm of chorionic plate
and in the connecting stalk.
13.
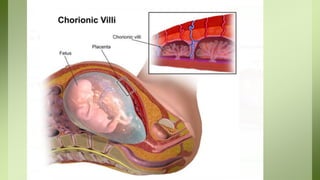
Parts of thechorion :
As a result of increase in the size of chorionic vesicle the
chorion is differentiated into two parts:
1) Chorion frondorsum: The villi which cover the embryonic
pole of the chorionic vesicle (opposite the decidua basalis)
become more numerous and branched giving a leaf like
appearance and forming the fetal part of the placenta.
2) Chorion leave: As pregnancy advances, the villi which lie
over the remaining part of the chorionic vesicle begin to
degenerate and become smooth.
This part of chorion is in relation to decidua capsulation.
15.
Functional types ofchorionic villi:
1) Stem or anchoring villi:
these are tertiary villi which are attached directly to the
decidua basalis.
Function: fixation of the growing embryo to the uterine
wall.
2) Free of absorbing villi: arise from the sides of the
stem villus to flout inside the inter villus spaces.
Function: Exchange of nutrient material and gases
between fetal and maternal blood occurs through them.
The amnion:
is amembrane attached to the periphery of the
embryonic disc.
it is continuous with the ectoderm and bounds the
amniotic cavity.
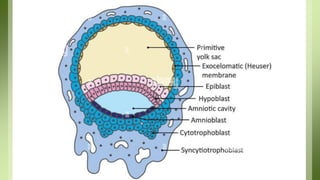
Development of amnion and amniotic cavity
The amniotic cavity appears during
implantation of the blastocyst, as small clefts between the
ectoderm of the inner cell mass and the trophoblast these
clefts joined together, forming small space called the
20.
A layer oflarge flattened cells called the
amnioblasts develop from the inners surface of the
trophoblast limning the amniotic cavity and
become continuous with the ectoderm.
The roof the amniotic cavity is formed by the
amnioblastic cells, while the floor is formed by the
primary ectoderm.
The amniotic cavity increase in size, the layer of
the amnioblasts loses its contact with the inner
surface of trophoblast.
The space between the outer surface of the
amnion and the inner surface of the trophoblast
becomes filled with extraembryonic mesoderm.
22.
Large cavities appearin the extra-embryonic mesoderm.
Then fuse to form large space called extra-embryonic coelom.
At first the cavity is small and transient
After folding, the embryo grow, the amniotic cavity expands
and surround the whole fetus, and the amnion and chorion
become fused
also the body stalk and yolk sac stalk become approximated to
form the umbilical cord, by this means the umbilical cord
acquires an outer covering of amnion.
24.
The amniotic cavitycontains a pale straw coloured watery fluid,
the liquors amnii.
At the end of pregnancy the fluid is normally from 750-1500 ml.
Source of amniotic fluid:
1- Amniotic epithelium.
2- Excretion of fetal kidneys.
3- Transudation of filtration from the placenta.
Later in pregnancy, the amniotic fluid is probably absorbed
into the fetal circulation and then transferred to the mother via
the placenta.
25.
Functions:
1- It allowsfetal movement and help proper development of
musculoskeletal system of the fetus.
2- It forms hydrostatic bag around the fetus protecting it
from external shocks.
3- It prevents adhesions between different parts of the fetus.
4- It may be a source of nutrition because it contains glucose,
amino acids and some minerals.
5- It provides a space where urine and meconium accumulate
before birth.
6- It provides an equal pressure on all parts of the embryo;
this allows symmetrical development of the different parts of
the embryo.
26.
7- It keepsthe fetal body temperature constant.
8- In the first stage of labour, the amniotic fluid dilates the cervix.
9- It is an aseptic medium surrounding the fetus, when the
membranes rupture, the amniotic fluid washes the vagina before
delivery of the fetus.
Anomalies of amnion:
1- Oligohydramnios: When the volume of amniotic fluid is less
than 500 ml, this may be due to renal agenesis (absence of
kidneys).
2- Polyhydramnios: When the volume of amniotic fluid is more
than 1200 ml.
The yolk sac:
is a cavity develops on the ventral aspect of the
embryonic disc.
There is a primary, a secondary and a definitive yolk sac.
1- The primary yolk sac:
It lies ventral to the embryonic plate; its roof is formed
by the primary entoderm.
Its remaining walls are formed by the heuser's
membrane (flat cells delaminated form the inner surface
of the cyto-trophoblast).
31.
This membrane iscontinuous with the entoderm.
The primary yolk sac then separates itself from the trophoblast
by the development of the extra-embryonic coelom.
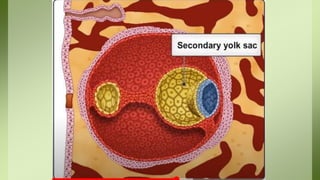
2- The secondary Yolk sac:
In the chorionic vesicle stage, the yolk sac decreases in size, its
roof is formed by the primary entoderm, its wall is formed by
the exacoelomic membrane (heuser's membrane).
A finger like diverticulum extends from the dorso-coudal part
of the secondary yolk sac into the substance of the connecting
stalk.
This is the allantoentric diverticulum.
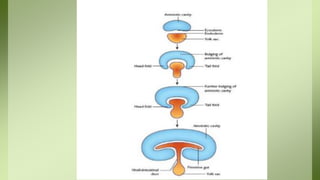
33.
3- The definitiveyolk sac:
As a result of folding at the embryonic disc, the dorsal
part of the secondary yolk sac is enclosed in the
embryo to form the gut which is divided into:
1- Foregut: in the head fold.
2- Hindgut: in the tail fold.
3- Mid gut: in between.
35.
The remaining partof the yolk sac outside the embryo is called the
definitive yolk sac.
The communication between the gut and the definitive yolk sac becomes
narrowed and elongated to form the yolk sac stalk (or vitello-intestinal
duct).
When the amnion expands, the vitello-intestinal duct is incorporated
inside the umbilical cord.
The yolk sac shrikes into a small vesicle which lies under the amniotic
covering of the placenta close to the attachment of the cord.
The vitellointestinal duct is obliterated, fibrosed and degenerated.
36.
Anomalies of theyolk sac
1- The proximal end of the vitello-intestinal duct may persist forming
Meckl's diverticulum, it is one of most common malformation of the
digestive tract.
-The diverticulum occurs in 2-4% of cases is appears as a fingers-like
pouch about 3-6 cm. long, arising from the anti-mesenteric border of the
ileum 40-45cm. from the ileocaecal junction.
2- The vitello-intestinal duct may be fibrosed and may persist as a
fibrous ligament connecting the intestine to the umbilicus.
3- The vitello-intestinal duct may remain patent: in this case the
umbilicus is discharging faecal matter after falling of the umbilical
stump. This condition is called congenital faecal umbilical fistula or
vitelline fistula
37.
4- Meckl's diverticulummay be connected to the umbilicus
by a fibrous cord (persistent vitello-intestinal ligament). It
may lead to twisting of the intestine and its obstruction.
5- Umbilical sinus due to persistence of vitello-intestinal duct
near the umbilicus.
6- Vitelline cyst due to non-obliterated part of vitello-
intestinal duct and the remaining of the duct is fibrosed and
persist as fibrous band.