This document discusses finger clubbing, the Glasgow Coma Scale (GCS), and muscle power grading. It provides details on:
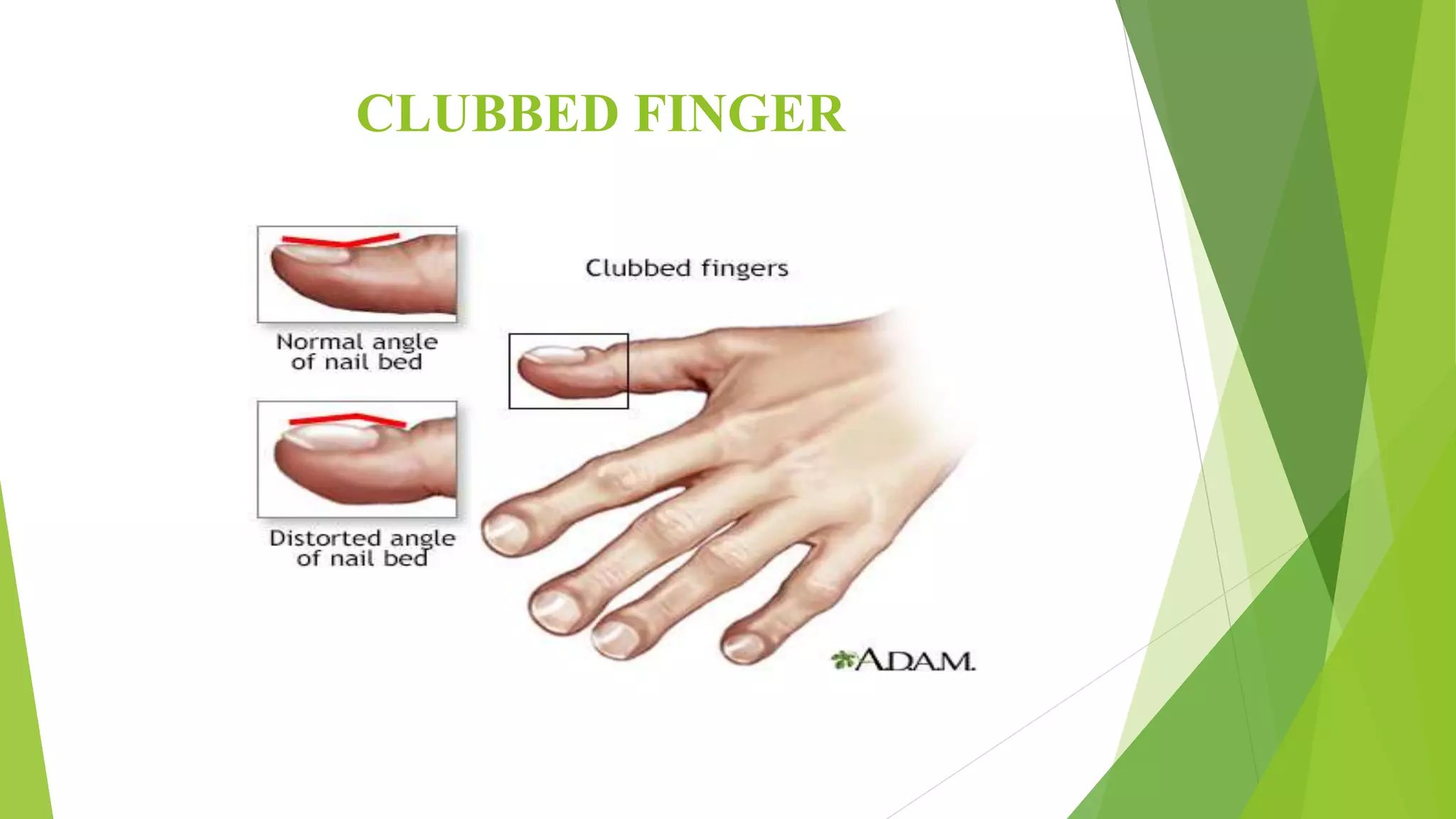
1) The anatomy, causes, clinical presentation, and grading of finger clubbing. Clubbing can be idiopathic or secondary to underlying conditions like lung and heart diseases.
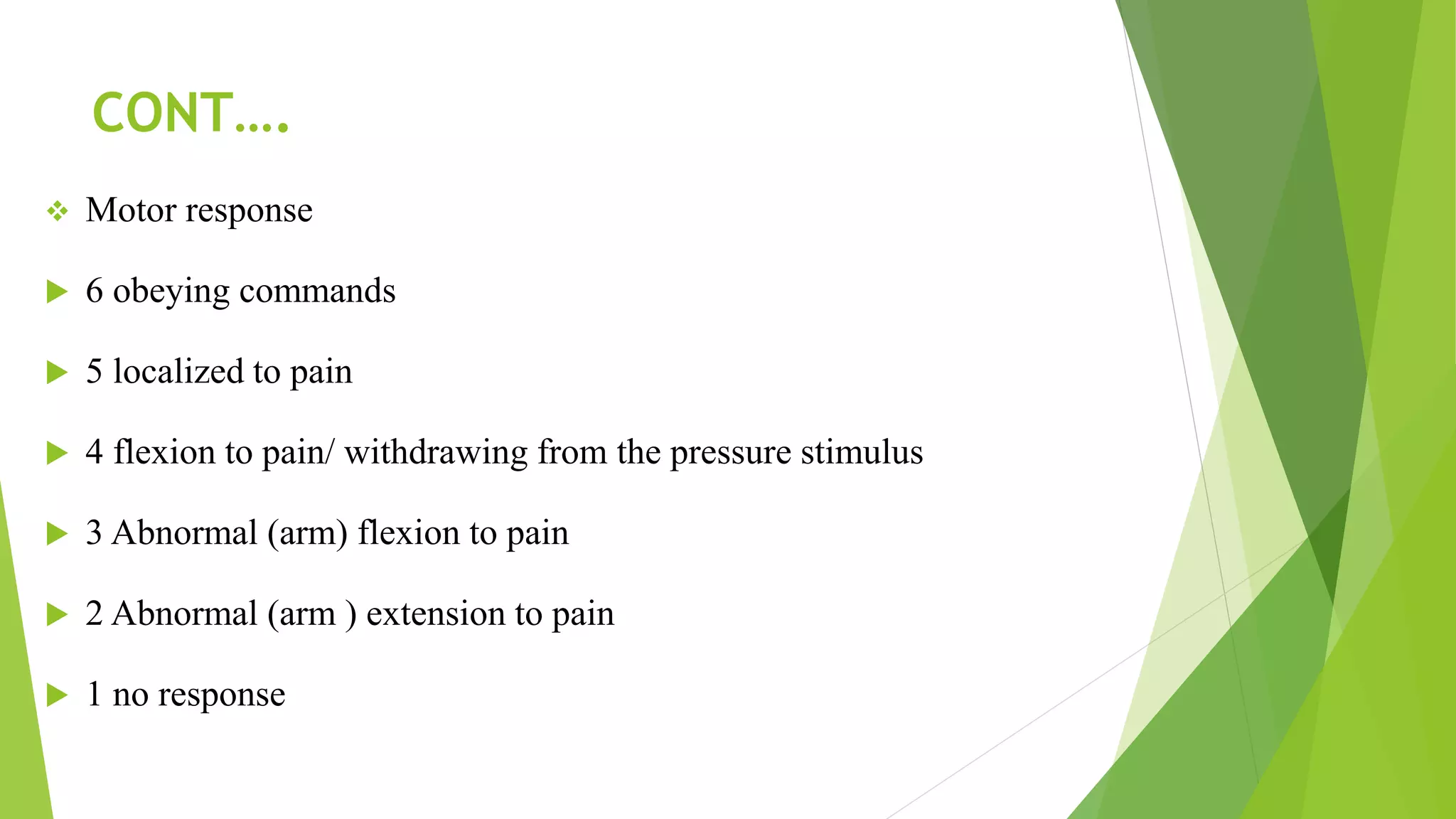
2) The GCS, a neurological scale used to assess consciousness on a 3-15 scale. Scores indicate severity of brain injury and can be influenced by baseline status, sedation, and injury.
3) Muscle grading using the Oxford Scale from 0-5, to assess strength, power, and endurance of muscles like the shoulders, elbows, and hips. Grading