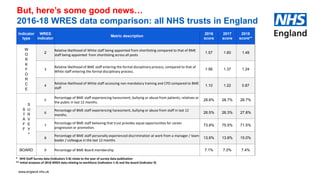
The Muslim Network Health Collaboration focuses on addressing health inequalities within the NHS, emphasizing diversity and inclusion, particularly regarding Black and Minority Ethnic (BME) representation among staff. The document discusses various initiatives supporting health engagement within the Muslim community, shared personal stories related to Hajj, and the significance of key Islamic practices such as Hajj and Eid. Additionally, it highlights ongoing efforts in cancer screening and public health programs as they relate to improving health outcomes for underserved populations.
















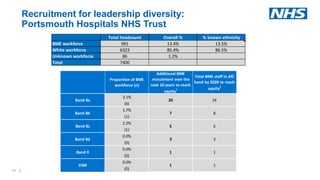









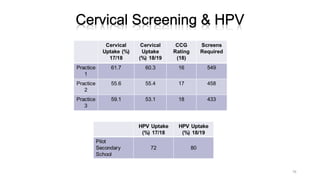
![Cancer Screening (Our Findings)
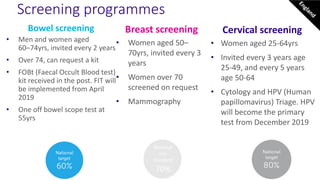
• Reported increased understanding of process, and intention to
partake in NHS screening programs after attending intervention
• [Intra]Faith and cultural sensitivity crucial (music, fate, segregation)
• Need to understand & engage with health behaviors and beliefs
of mosque population](https://image.slidesharecdn.com/muslimnetworkhajjevent2019-190930091557/85/Muslim-Network-Hajj-Event-2019-69-320.jpg)

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





