1) Public Health England (PHE) is launching an inequalities strategy and toolkit to address unfair barriers to accessing screening programs and to help individuals make informed choices about screening.
2) The strategy builds on past work and stakeholder input, and seeks to provide leadership, evidence, and tools to identify and address screening inequalities at local levels.
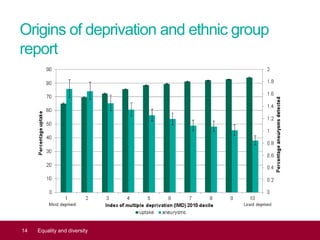
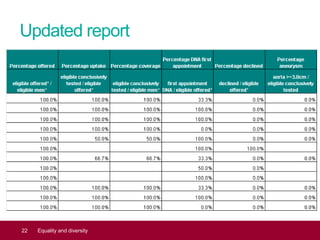
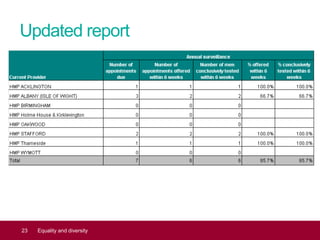
3) A key part of this effort is a new report analyzing screening data based on deprivation, ethnicity, and other factors to help benchmark progress on reducing inequalities.