
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Female Genital System
Similar to Female Genital System (20)
Recently uploaded
Recently uploaded (20)
Female Genital System
- 2. CHAPTER 22CHAPTER 22 DISEASES ofDISEASES of OVARIESOVARIES PREGNANCYPREGNANCY PLACENTAPLACENTA
- 3. DISEASES of OVARIES• DEGENERATIVE? • INFLAMMATORY? • CYSTS • TUMORS – Müllerian (“Germinal”) – Germ Cell – Sex Cord/Stromal – Metastatic
- 4. DISEASES of PLACENTA • ANOMALIES • “BENIGN” tumors (MOLES) • MALIGNANT tumors (CHORIOCARCINOMA)
- 8. Everything you can see or feel is lined by serosa (i.e., mesothelial cells, visceral and parietal
- 11. TERMS• “Germinal” Epithelium (Mesothelium) • Ovum (Oocyte) • Tunica Albuginea • Primordial Follicle • Primary Follicle • Mature “Graffian” follicle (antral or secondary) • Granulosa cells ( Estrogen) • Thecal cells ( Estrogen) • Corpus luteum ( Progesterone) • “Atretic” follicle • Corpus Albicans • “Stroma”
- 16. B=GRANULOSA D=THECA INTERNA E=THECA EXTERNA
- 19. ESTROGEN • Controlled by FSH and LH • Develop, Lactate Breast Lobules • Proliferate Endometrial Glands • “Cardioprotective” • “Bone Mass” protective
- 20. PROGESTERONE • Controlled by FSH and LH • SECRETE Endometrial Glands • IMPLANTATION of the blastocyst • Lactation
- 24. POLY-Cystic Ovarian Disease (Stein-Leventhal syndrome) 5% Prevalence Anovulation Oligomenorrhea Obesity Hirsutism
- 26. OVARIAN TUMORS • MÜLLERIAN (MAJORITY) – Serous (Benign, Borderline, Malignant) – Mucinous (Benign, Borderline, Malignant) – Endometroid (Benign, Borderline, Malignant) – Adenosarcoma (Carcinoma AND Sarcoma) – Mesodermal Mixed (MULTIPHASIC Sarcoma) – Clear Cell – Brenner (almost always benign) – Transitional (almost always look like Brenner) • Germ Cell (Not surprisingly, like males) • SEX-CORD/STROMAL • METASTATIC
- 27. OVARIAN TUMORS • Solid vs Cystic • Functional vs. NON-functional • Benign vs. Malignant • First clinical presentation may be ascites • Malignant ascites in a woman is ovarian cancer until proven otherwise • CA-125 is THE important tumor marker in ovarian cancer, especially as a follow up.
- 28. SEROUS, BENIGN
- 29. MUCINOUS, BENIGN
- 33. PSAMMOMA bodies are dried up papillae of papillary adenocarcinomas, usually in the thyroid, but in ANY papillary adenocarcinoma
- 35. OTHER MÜLLERIAN • ENDOMETRIOD, malignant – (looks like endometrium) • CLEAR CELL, malignant – (clear cells, reminiscent of renal clear cell ca.) • CYSTADENOFIBROMA, benign – (BENIGN “FIBROUS” COMPONENT) • BRENNER TUMOR, benign – (transitional cell nests) • CARCINOMA with SARCOMA – (adenosarcoma, mixed Müllerian)
- 36. “GERM CELL” Tumors • Teratomas (usually benign in ovary), i.e., “mature” cystic teratoma or dermoid cyst • “Immature” teratomas are regarded as malignant • Dysgerminoma (look exactly like the testicular seminoma), malignant • Endodermal Sinus (Yolk Sac), malignant, Just like testicular • Choriocarcinoma, malignant, just like testicular
- 42. ENDODERMAL SINUSENDODERMAL SINUS TUMOR, akaTUMOR, aka YOLK SAC TUMORYOLK SAC TUMOR
- 43. CHORIOCARCINOMA,CHORIOCARCINOMA, Just like testis or placentaJust like testis or placenta
- 44. SEX-CORD/STROMAL TUMORS • Chiefly benign and NON-cystic, i.e., “solid”, often functional (hyper-estrogen-ism) • Granulosa-Theca • Fibroma-Theca • Sertoli-Leydig (Androblastoma)
- 46. B=GRANULOSA D=THECA INTERNA E=THECA EXTERNA
- 48. DISEASES of PREGNANCY •EARLY Pregnancy •LATE Pregnancy
- 49. EARLY PREGNANCY • SPONTANEOUS ABORTION • ECTOPIC PREGNANCY
- 50. Spontaneous Abortion • 15% - 35% • Fetal Causes –Usually Genetic • Maternal Causes (placental, uterus infections or trauma) –Toxo, Mycoplasma, Listeria –Trauma
- 51. Ectopic Pregnancy • Chiefly TUBAL, but ovarian or abdominal rare •1% OF NORMAL WOMEN •35%-50% OF WOMEN with previous SALPINGITIS/PID • + HCG, Abdominal pain, 1st trimester, ultrasound
- 53. LATE PREGNANCY • PLACENTAL ANOMALIES • TWIN PLACENTAS • PLACENTAL INFLAMMATIONS • TOXEMIA (ECLAMPSIA/PRE- ECLAMPSIA) • INTRAUTERINE GROWTH RETARDATION
- 54. PLACENTAL ANOMALIES • Accessory Lobes • Bipartite Placenta • Circumvallate Placenta • Placenta Accreta, chorion going DIRECTLY to the myometrium
- 58. CIRCUMVALLATE
- 59. PLACENTA ACCRETA NO DECIDUA BETWEEN VILLI AND MYOMETRIUM
- 60. MRI of Placenta PREVIA, or LOW-LYING placenta, usually anatomically normal, but just lies LOWER than it should.
- 62. TOXEMIA of PREGNANCY (PRE-eclampsia) • Hypertension • Proteinuria • Edema • Related to Placental Ischemia • Risk for DIC, convulsions (eclampsia)
- 63. Intrauterine Growth Retardation • Fetal causes: Genetic, malformations • Maternal Causes, vascular diseases, toxemia, infections, placental diseases • Placenta size (350-700g) ~ Fetal size (7.5 lb)
- 64. Placental Infections • Villitis vs. chorionamnionitis vs. funisitis • ASCENDING vs. hematogenous • ASCENDING are usually bacterial, and chorionamnionitis • HEMATOGENOUS are often TORCH, and villitis
- 65. Placental Neoplasms, i.e. gestational trophoblastic disease • Benign: MOLES (Hydatidiform moles) • Malignant: CHORIOCARCINOMA • BOTH are associated with increased or persistent levels of the placental hormone HCG
- 67. Hydatidiform Mole • 1/1000 in USA • 1% in Indonesia • Also called NON-invasive mole in its most common benign variant, but can also be “invasive” • Complete (2% chorioCA incidence) or partial (0% incidence) • Grapelike clusters, i.e., swollen villi
- 69. The MAIN thing differentiating benign from malignant from worrisome trophoblastic neoplasms is INVASIVENESS of the trophoblast
Editor's Notes
- Primary germ cells, male or female, first arise in the yolk sac and migrate to the genital ridge, which is in close proximity to the mesonephros. Eventually, retroperitoneal testes migrate through the inguinal canal to the scrotum, covered by peritoneum. Ovaries stay in the pelvis, and are covered by serosa, and are therefore intraperitoneal, but POSTERIOR to the fallopian tubes.
- The CORTEX is the site of developing follicles. The MEDULLA is relatively free of developing follicles, and rich in connective tissue (stroma) and blood vessels.
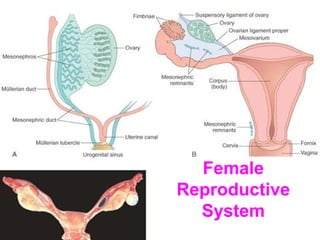
- Major internal female genitalia structures, landmarks, and interrelationships. In which ligament does the ovarian artery lie? Through which structure does the round ligament travel. Normally the uterus is a bit ANTE-VERTED and ANTE-FLEXED
- Major internal female genitalia structures, landmarks, and interrelationships.
- GREAT whole mount to demonstrate overall cortex vs. medullary differentiation.
- OOCYTE PRIMORDIAL FOLLICLE (simple squamous covering) PRIMARY FOLLICLE (cuboidal epithelial covering)
- Zona pellucida, arrow, becomes “atretic” follicle. Is this a primary follicle? Ans: YES Why?
- Secondary = Graffian = Antral follicle Where is the antrum?
- Find the cumulus oophorus, liquor folliculi, and corona radiata
- Granulosa and theca INTERNA cells make estrogen.
- LUTEAL cells, under LUTEINIZING hormone and FSH too, make progesterone. LUTEUM means YELLOW. Why? Why is ANYTHING bright yellow? A corpus luteum of pregnancy is considerably larger than a regular, NON-pregnancy, corpus luteum, often, perhaps about a half or third the size of the ovary.
- Corpus albicans. ALBA means WHITE. Why is it white?
- Most common PRE-menopausal cyst
- Any EXTREMELY yellow cyst of a premenopausal ovary, is regarded as luteal in origin. Very common PRE-menopausal cyst
- Although the cortical area of the normal ovary contains cysts, i.e., various stages of follicular development, true PCOD (PolyCystic Ovarian Disease, or Stein-Leventhall) ovaries are BIGGER (2x) than normal premenopaosal ovaries and have “true” cysts, NON-ovulatory, NOT just stages of follicular development. Is a “cyst” a “tumor” (i.e. swelling) in the classical sense of the word, like a bump on the head. Is a cyst usually a true neoplasm? Ans: Of course not!
- Always think of true ovarian tumors as following the normal anatomy/histology in these FOUR groups---mullerian, germ, sex-cord, metastatic. In contrast to the testicle, the ovary DOES occasionally get metastases.
- Gross, microscopic, physiologic, behavioral classification factors for ovarian tumors.
- The HUGEST tumors ever reported in human beings (50-100 lbs.?) are frequently benign mucinous ovarian tumors.
- Q: What other adjective can we give to this tumor besides serous? Ans: Papillary
- Close up of papillae
- Why is this serous and NOT mucinous?
- PSAMMOMA bodies
- Less common Müllerian carcinomas
- I TOLD you this looks the same as TESTICULAR germ cell tumors.
- Dermoid “cyst” = BENIGN CYSTIC TERATOMA, BY FAR the most common ovarian NEOPLASM of younger women, usually BENIGN
- Whether the teratomatous elements are “mature” or “immature” determine, greatly, the behavior of the teratoma, i.e., benign or malignant.
- IMMATURE looking neural tissue. This is much more likely to behave badly (i.e., malignant) than a mature one. Often, you might see retinal tissue, like you see here.
- Female dysgerminomas are IDENTICAL in appearance to male seminomas, i.e., germ cells + lymphocytes. You’d have to tell the pathologist whether this was a male or female in order for him to diagnose seminoma vs. dysgerminoma.
- Schiller-Duvall Body, just like in the testis yolk sac tumor!
- EXACTLY the same as a malignant HCG producing testicular choriocarcinoma or a malignant HCG producing placental choriocarcinoma
- “Sex cord” = “stroma” MANY are functional, i.e., associated with hyper estrogenism (or androgenism)
- Call-Exner bodies are virtually diagnostic of granulosa cell tumors. Q: Do they remind you of “rosettes”? Ans: YES
- Q: Would a “thecoma” derived from theca INTERNA be more likely to be functional than a thecoma derived from theca EXTERNA? Ans: YES Why? Note the “theca” has both a vesicular and spindle cell appearance. The juicy vesicular cells, theca interna, and tumors derived from them, can secrete estrogen. The spindly theca externa cells, usually do not, and may look simply like fibromas.
- Many thecomas look white and fibrous, That is why the term fibrothecoma is often used? Is a fibrothecoma or fibroma less likely to be functional than a thecoma? Ans: YES Why? Ans: It is derived from NON-estrogen producing cells.
- Accessory placental lobe. An extreme lobe might be called a BI-partite placenta.
- In a circumvallate placenta the amnionic, i.e., amniotic, membranes “thicken” or “double back”
- You might guess this kind of placenta would be VERY difficult to remove, and remnants (retained POC) might result in endometritis
- And don’t forget placenta “abruptio” or premature separation of placenta with hemorrhage (i.e., hematoma)
- Twin zygosity (mon- or di-) is related to the number of CHORIONS, NOT amnions or umbilical cords!
- Toxemia of pregnancy occurs in an amazing 6% of all pregnancies. Toxemia is also called PRE-eclampsia. When PRE-eclampsia is particularly severe and associated with more serious systemic effects such as DIC or convulsions, it is called ECLAMPSIA.
- What does TORCH stand for? T-oxo O-ther R-ubella C-MV (Do you see the BASOPHILIC intranuclear inclusion in the above villitis pic?) H-erpes
- Syncytial cells are FUSED, CYTO-trophoblastic cells are deeper stem cells. Is this chorionic villus mature or IM-mature? Ans: mature Why? Ans: It has blood vessels in its core. If it was IMMATURE, it would NOT need secondary blood vessels and can diffuse oxygen and nutrients WITHOUT secondary blood vessel formation.
- In COMPLETE moles, ALL the villi are swollen. They turn into choriocarcinomas 2% of the time. In PARTIAL moles, only some are. They NEVER turn into choriocarcinomas.
- NOTE trophoblast looks NORMAL, i.e., NON-invasive and NON-proliferative, and NON atypical.
- Choriocarcinoma. Note invasive trophoblast.
- Choriocarcinoma. Note extreme pleomorphism of trophoblastic cells.