Downloaded 16 times
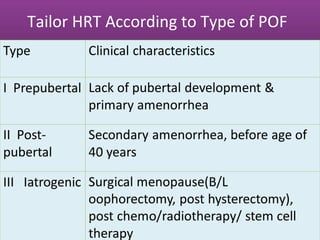
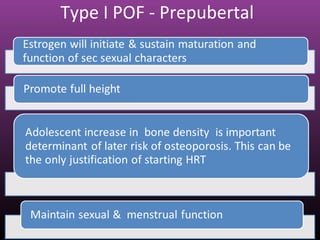
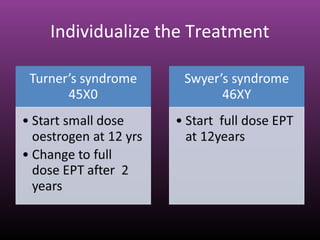

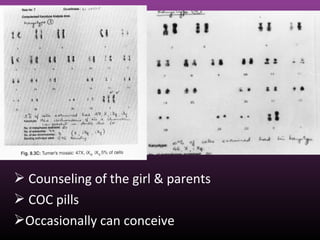

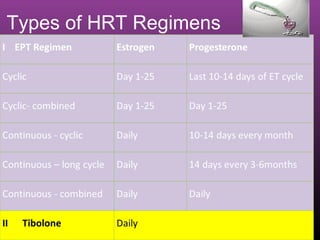
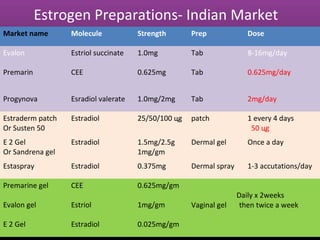
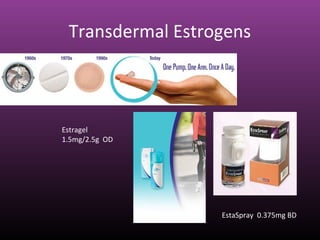
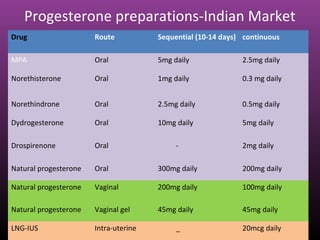
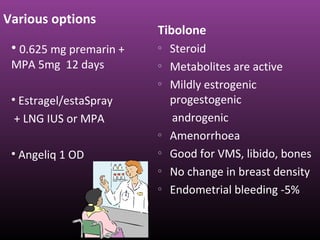
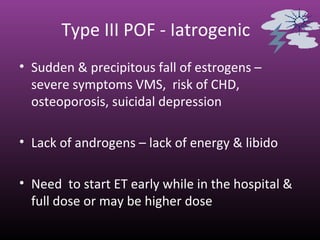

This document discusses hormone replacement therapy for premature ovarian failure. It notes that HRT for POF is true replacement therapy rather than extension therapy. It should be started at diagnosis and continued until natural menopause to avoid long-term ill effects. The document outlines different types of POF and tailoring HRT to each type. It provides details on estrogen and progesterone preparations available in India and various HRT regimens and options for POF.