Download to read offline

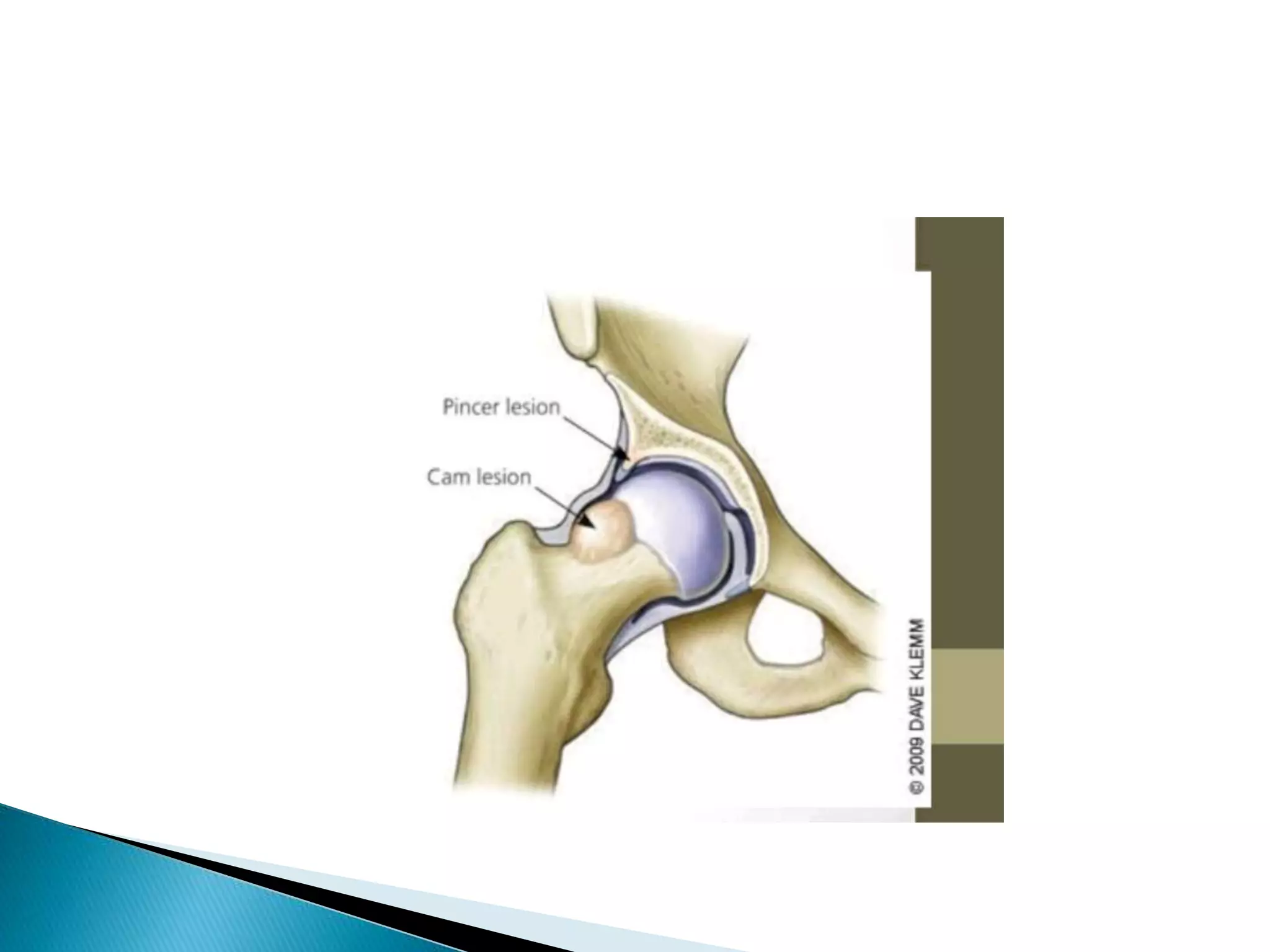






























This document discusses hip impingement, including pincer and cam types. It describes the normal anatomy of the hip joint and how impingement arises from uneven surfaces of the femoral head or acetabulum. Common symptoms include groin pain and limited range of motion. Diagnosis involves physical exam, x-rays to evaluate bone shapes, and MRI to view soft tissues. Treatment options range from physical therapy for mild cases to open surgical correction of bone deformities or hip replacement for advanced arthritis.

































![Femoroacetabular%20 impingement[1]](https://cdn.slidesharecdn.com/ss_thumbnails/femoroacetabular20impingement1-130422051258-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)