Download to read offline

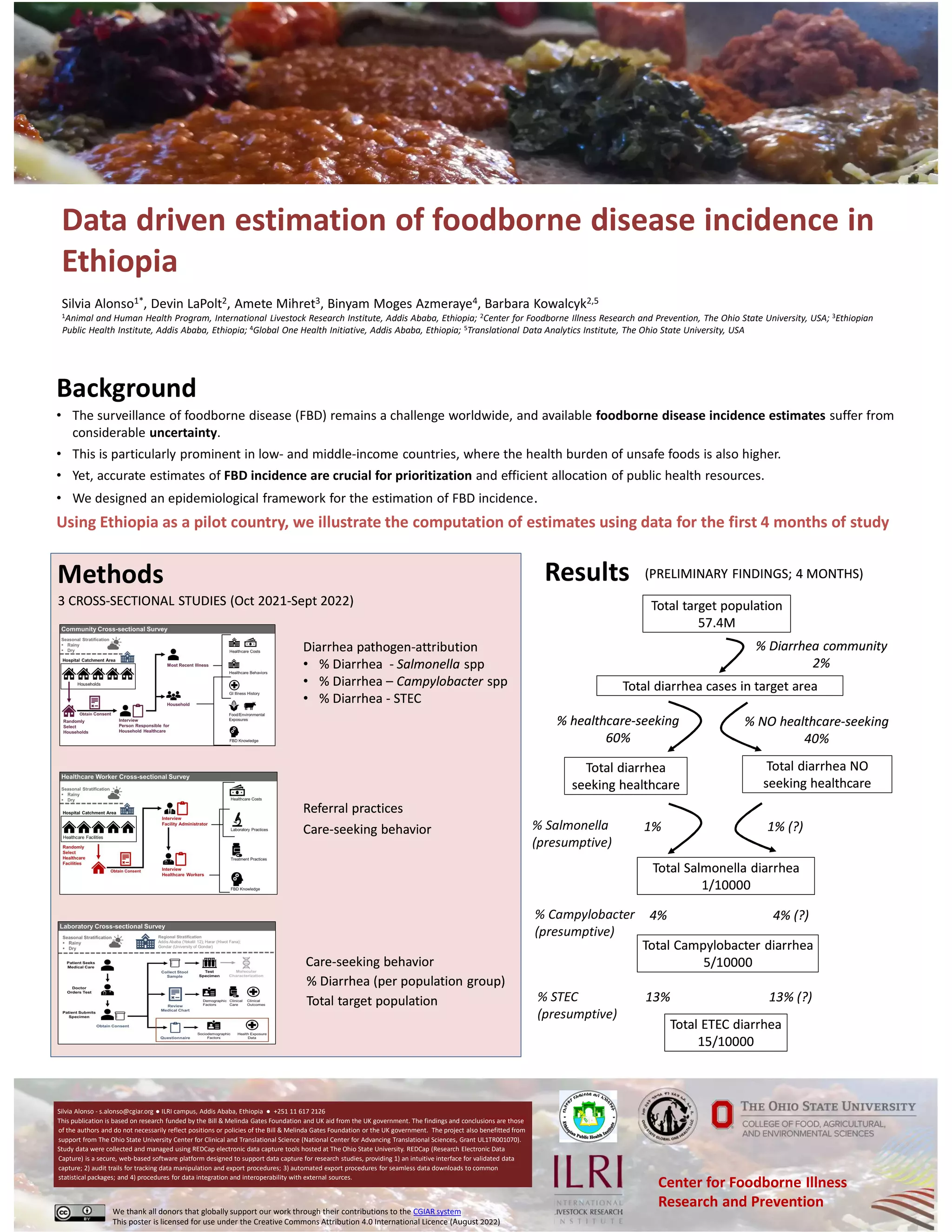

The document discusses the need for accurate estimation of foodborne disease incidence in Ethiopia, highlighting that existing estimates are uncertain, especially in low- and middle-income countries. An epidemiological framework was developed to compute incidence estimates, supported by data from three cross-sectional studies conducted between October 2021 and September 2022. The research received funding from the Bill & Melinda Gates Foundation and UK aid, utilizing the REDCap platform for data management.



































































