• INTRODUCTION
• STEPSFOR ACHIEVING COMPLETE DENTURE ESTHETICS
1. Examination
2. Accurate impression
3. Jaw relation
4. Selection of anterior teeth
5. Arrangement of teeth
6. Characterization of denture
• ESTHETICAL ERRORS
• CONCLUSION
CONTENT
2
3.
• Edentulism isa long-term handicap that makes it difficult for edentulous people to do
basic functions like eating, speaking, and socializing.
• As a result of these deficits, some individuals may experience increasing social and
psychological problems.
• Tooth loss also has physical implications, such as atrophy of the supporting alveolar
tissues, loss of facial muscle support, and decreased biting force and masticatory
efficiency
INTRODUCTION
2
4.
• Dentures restorea natural appearance in our image-conscious world, resulting in enhanced
patient confidence and ease in social interactions.
• Esthetics in Complete denture is not only the exact selection of teeth but the lost facial
anatomy. Facial esthetics thus play a critical role
• Cheeks are usually the most visible region of the face, supported by teeth, ridges, and
muscles, and so play an important role in facial aesthetics.
• Concavities and hollowing of the cheeks are caused by the loss of molars, total
Edentulism, an age-related decrease in muscular tone, and weight loss
5.
• One ofthe objectives in complete denture prosthetics is to produce a
harmonious appearance of the denture when in the patient’s mouth.
• A denture usually perceived as esthetics when the teeth and bases are in
harmony with the facial musculature as well as the size & shape of the
head.
• The subject of esthetics should be examined from 3 points of view
biological - physiological, biomechanical and psychological.
6.
Physiological
• It isnecessary to have an understanding of facial musculature, normal facial appearance,
and the physiological limits within which esthetic compromises are to be made. A proper
impression procedure is necessary to provide the dentist with a final maxillary cast that has
an accurate representation of the labial vestibule and all of the other remaining structures.
7.
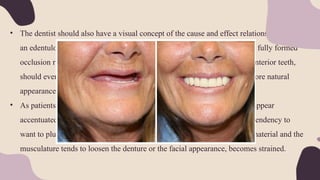
• The dentistshould also have a visual concept of the cause and effect relationship. eg: If
an edentulous patient has a tight, drawn & thin lips, proper support with a fully formed
occlusion rim and lip support by the labial 2/3 of the artificial maxillary anterior teeth,
should evert the vermillion border of the lip. This would afford a much more natural
appearance
• As patients become older the natural lines of farce tend to deepen and to appear
accentuated and the elasticity of the facial musculature is lost. There is a tendency to
want to plump out the face with additional thickness of the denture base material and the
musculature tends to loosen the denture or the facial appearance, becomes strained.
8.
• Another approachto removing facial wrinkles is to Increase the VD. This approach is
fraught with the greatest of dangers and must be used with caution. The actual process of
trial placement of the maxillary anterior teeth and the function of the maxillary and
mandibular anterior during the production of speech gives one of the best guidelines for
creating and maintaining an adequate inter occlusal distance.
9.
• The followingprinciples should be followed in the placement of anterior teeth.
1) The lower anteriors should be placed lower in order to maintain an adequate interarch
space. This will necessitate lowering of the occlusal plane posteriorly. This will have the
effect of placing the teeth closer to the mandibular ridge giving stability to the lower
denture.
2) The maxillary teeth should be moved slightly more anteriorly at the incisal edges. Tilting
the incisal edges of the mandibular incisors; lingually should be avoided. According to
Muysigmes for every 1 mm the incisal edges of the mandibular anterior teeth are posterior to
their normal arrangement, the tongue is deprived of approximately 100cub mm of space in
which to function.
10.
Biomechanical
• There arecertain mechanical limitations in the placement of anterior teeth that must be
taken into account. The anterior teeth should be placed closely in relation to the residual
ridge as were the original natural teeth. Fish says the proper position for the teeth is not
necessarily on the ridge, inside the ridge, or outside the ridge, but at a point where the
tongue and cheek pressures balance.
11.
Psychological
• Patient's selfimage is an important factor in esthetics. A patients perception of his or her
appearance may result in a broad simle (if it is a positive self evaluation.) or a tight lipped,
small, controlled smile, A patient with a poor self image may appear done, unsure,
questioning and introverted,. A patient with a more positive feeling tends to smile more
broadly.
12.
1. Examination
2. Accurateimpression
3. Jaw relation
4. Selection of anterior teeth
5. Arrangement of teeth
6. Characterization of denture
STEPS FOR ACHIEVING COMPLETE
DENTURE ESTHETICS
13.
EXAMINATION
• Careful evaluationof mental attitude.
• Preconceived hopes and desires should be determined.
• Emotional response regarding esthetics - attitude of indifference to demanding.
• This mental harmony between patient and dentist must exist or failure is inevitable
14.
ACCURATE IMPRESSION
• Asteeth are lost, functions of facial muscles are impaired.
• Resultant edentulous appearance has profound influence on patient.
• Supporting the facial muscles with properly formed borders is essential.
• A long standing edentulous patients requires thicker borders.
15.
• Natural appearanceof the lips in relation to the base of nose is of prime
significance.
• Improperly contoured labial border will lead to tenseness and extreme fullness of
lip.
• Overcontoured border will lead to denture displacement.
• Thus the impression visit is an appearance phase visit.
16.
JAW RELATION
• Asteeth are lost, functions of facial muscles are impaired.
• Labial surface of maxillary rim provides fullness required to support the upper lip
naturally in repose and function.
• Resorbed maxillary ridge form should not be used to control the anteroposterior
position of the wax. Rather it should be adjusted with consideration for the
orbicularis oris muscle and the muscles attached to it.
17.
• Correct placementof the occlusal plane is important with respect to denture
stability, function, and esthetics .
• The occlusal plane should be half way between maxillary and mandibular ridges.
• Maxillomandibular opening- occlusal vertical dimension is responsible for the
harmony between the lower third of the face and the face as a whole.
• Vertical dimension and centric relation are closely interrelated, and loss of vertical
dimension results in a more exaggerated class III occlusion and facial appearance.
18.
• establishing anacceptable vertical length of face is a fundamental esthetic
concern.
• An excessive VD leads to strained and artificial appearance.
• Insufficient VD leads to changes characteristic of aging process as chin comes too
close to nose, compresses upper lip at centre and drooping of corners of the
mouth, producing a thin upper lip and prominent lower lip
• The final VDO must not be determined by pleasing facial proportions alone, since
this would lead to excessive VD and subsequent bone resorption.
• At best, an interocclusal distance must be provided within physiological limits and
individually determined
19.
TEETH SELECTION
• Theselection of artificial teeth & their arrangement to meet esthetic requirements
demand artistic skill in addition to scientific knowledge.
• There are no rules of thumb for this procedure , however, there are anatomic
landmarks & manufactured aids if adhered to, will result in esthetically pleasing
complete dentures that are also functional.
• The goals for this phase of therapy are to construct complete dentures that:
1. Function well,
2. Allow the patient to speak normally,
3. Are esthetically pleasing, &
4. Will not abuse the tissues over residual ridges
20.
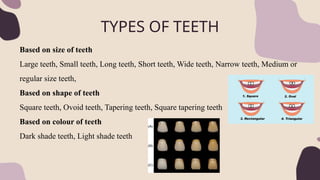
TYPES OF TEETH
Basedon size of teeth
Large teeth, Small teeth, Long teeth, Short teeth, Wide teeth, Narrow teeth, Medium or
regular size teeth,
Based on shape of teeth
Square teeth, Ovoid teeth, Tapering teeth, Square tapering teeth
Based on colour of teeth
Dark shade teeth, Light shade teeth
21.
TYPES OF TEETH
Anatomicteeth (Cusp teeth)
i. With 33° cuspal angulation.
ii. With 30° cuspal angulation.
Semi-anatomic teeth (Low cusp teeth)
i. With 20° cuspal angulation.
ii. With 10° cuspal angulation.
Non anatomic teeth (Cuspless teeth)
i. with 0° cuspal angulation (mono plane teeth).
22.
TYPES OF TEETH
Acrylicteeth Porcelain teeth
Composite
teeth
Porcelain acrylic
combination
scheme
Acrylic teeth
with amalgam
inserts
Acrylic teeth
with gold
occlusal surface
23.
ANTERIOR TEETH SELECTION
Guidesfor the anterior teeth selection:
1.Pre-extraction guides.
2.Examination of existing dentures.
3.Indirect methods of tooth selection (post extraction guides).
Study cast- theseare the most reliable guides in selecting the size,
shape, & position of the artificial teeth.
26.
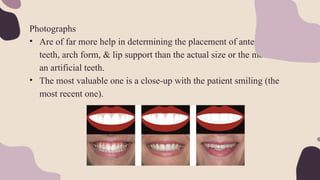
Photographs
• Are offar more help in determining the placement of anterior
teeth, arch form, & lip support than the actual size or the mould of
an artificial teeth.
• The most valuable one is a close-up with the patient smiling (the
most recent one).
27.
Radiographs - Cansupply information about the width, length, &
shape of the teeth to be replaced.
28.
Extracted teeth
• Theymay be utilized in selecting the size & mould of the
artificial teeth but are of little use in shade selection (because
of colour changes).
29.
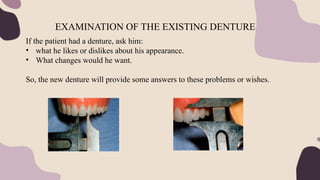
If the patienthad a denture, ask him:
• what he likes or dislikes about his appearance.
• What changes would he want.
So, the new denture will provide some answers to these problems or wishes.
EXAMINATION OF THE EXISTING DENTURE
30.
INDIRECT METHOD OFTOOTH SELECTION (POST EXTRACTION
METHOD)
a. Size. (width, length, & thickness)
b. Form
c. Shade.
d. Material.
31.
WIDTH OF ANTERIORTEETH
• Bizygomatic width.
• The buccolingual centers of hamular notches.
• the size & contour of the residual ridges.
• Corners of the mouth.
• Canine eminence.
• The width of the nose.
• Lateral surface of the nose.
• The incisive papillae.
• Maxillomandibular relations.
• Cranial circumference.
32.
• The widthof the 6 anterior teeth = Bizygomatic width3.3
• The width of maxillary central incisor = Bizygomatic width16
• Width of maxillary lateral incisor is 2 mm less than central incisor
• Width of maxillary canine is 1 mm less than central incisor
• Total width of mandibular anteriors = 4/5 X (Total width of maxillary
anteriors)
33.
THE BUCCOLINGUAL CENTREOF HAMULAR NOTCH
The width of the 6 anterior teeth= The distance between the buccolingual
centres of the hamular notch+5mm.
THE SIZE & CONTOUR OF THE RESIDUAL RIDGES
The size of the casts have a relationship to the size of the anterior teeth.
34.
CORNER OF THEMOUTH
The distal surface of many natural canines is positioned at he corner of the
relaxed mouth i.e. The width of the 6 anterior teeth = The distance measured
between the two commisures (angles of the mouth).
35.
CANINE EMINENCE
If welldefined; it’s distal aspect may be taken as the mesiodistal width of the maxillary
anterior teeth. Measure the distance from the distal of one canine eminence to the distal of
other canine eminence with a flexible ruler. The measurement obtained indicates the total
width of maxillary anterior teeth.
36.
WIDTH OF THENOSE
vertical parallel lines extending from the centre of the ala of the nose onto the labial
surface of the upper occlusion rim will give an indication of the position of the cusp tips
of the maxillary canines.
LATERAL SURFACE OF THE NOSE
An imaginary line drown along the lateral surface of the nose through the centre of the
brow line & contacting the lateral aspect of the ala to the labial surface of the upper
occlusion rim will give an indication of the position of the distal aspect of the canine
tooth
37.
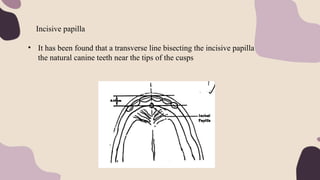
Incisive papilla
• Ithas been found that a transverse line bisecting the incisive papilla contacts
the natural canine teeth near the tips of the cusps
38.
MAXILLO MADIBULAR RELATIONSHIP
Anydisproportion in size between the maxillary and mandibular arches influences the
length, the width, & position of the teeth:
• In protruded mandibles ,the face is usually longer & require longer teeth
• If the mandibles are retruded, the mandibular anterior teeth are frequently smaller.
CRANIAL CIRCUMFERENCE
• The horizontal circumference of the cranium (about a plane passing through a glabella
& the maximum occipital point) is said to be 10 times the width of the maxillary
anterior teeth.
39.
Length of anteriorteeth:
• The vertical distance between the ridges.
• The lips
• The length of face
LENGTH OF ANTERIOR TEETH – INCISO GINGIVAL
LENGTH
40.
THE VERTICAL DISTANCEBETWEEN THE RIDGES
• The length of the teeth is determined by the available space between the
alveolar ridges.
• If the inter arch space is less then teeth with less inciso-gingival length
should be selected and in cases of more inter arch space, teeth with more
inciso-gingival length should be selected.
41.
THE LIPS :
•When the lips are relaxed & apart; the amount of the central incisors visible
below the lip is about 2-3mm in young person & less than half the amount in
an elderly patient.
• When the teeth are in occlusion & the lips are together; the labial incisal
third of the maxillary anterior teeth supports the superior border of the lower
lip.
• the incisal length or vertical composition of the anterior teeth: at rest (Frush
and Fisher).
young woman 3mm below lip line
young man 2mm below lip line
middle age 1.5mm below lip line
old age, 0 mm below to 2mm above lip line (Vig and Brundo)
42.
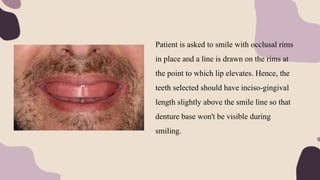
Patient is askedto smile with occlusal rims
in place and a line is drawn on the rims at
the point to which lip elevates. Hence, the
teeth selected should have inciso-gingival
length slightly above the smile line so that
denture base won't be visible during
smiling.
43.
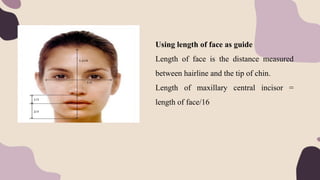
Using length offace as guide
Length of face is the distance measured
between hairline and the tip of chin.
Length of maxillary central incisor =
length of face/16
44.
The amount ofthe teeth which an individual shows varies depending on:
1. Length of the upper lip.
2. Mobility of the upper lip.
3. Vertical dimension of occlusion.
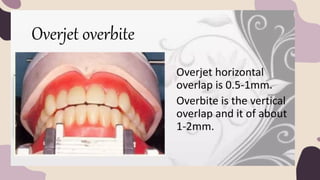
4. Vertical overlap (overbite).
45.
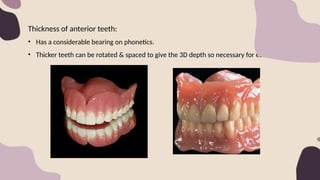
Thickness of anteriorteeth:
• Has a considerable bearing on phonetics.
• Thicker teeth can be rotated & spaced to give the 3D depth so necessary for esthetics.
46.
FORM OF ANTERIORTEETH
1. The form & contour of the face.
2. Shape of the edentulous maxillary arch.
3. sex.
4. Age.
47.
THE FORM &CONTOUR OF THE FACE.
• The shape of the anterior teeth should harmonize with the shape of the
patient’s face. (frontal & profile).
• Leon Williams (1914) claimed that , the shape of the maxillary central
incisor bears a definite relationship to the shape of the face.
• Leon Williams classified the form of the human face into:
1. Square.
2. Tapering. &
3. ovoid, or a combination of two or more of these basic forms
The method of tooth selection become known as the geometric theory.
48.
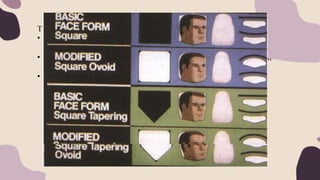
THE FORM &CONTOUR OF THE FACE.
According to Williams and House and Loop the shape of the teeth should be
inverse of the shape of the face.
The form of face is identified by connecting the following points on the lateral
aspect of face: the forehead, the zygomatic arch and the angle of mandible.
Accordingly, 3 basic forms of face and corresponding facial forms of teeth are
Square form
Ovoid form
Tapering form
49.
THE FORM &CONTOUR OF THE FACE.
Proximal Form of Teeth
Based on the profile of patient, proximal form of teeth can be-straight, convex
Incisal Form of Teeth
Based on the profile of patient, incisal form of teeth also can be-straight, convex
Curvature of Teeth
The tooth may curve in both mesiodistal direction and inciso gingival direction.
The mesiodistal incisogingival curvature of tooth selected should complement
the profile curvatures of the face.
50.
THE SHAPE OFMAXILLARY EDENTULOUS RIDGE
It was recognized that, there was some relationship between the Shape of the
edentulous maxillary arch & the maxillary teeth:
• V-shaped arch incisors narrower at the neck than at the incisal edge.
• Squarish arch parallel sided incisors.
• Rounded arch ovoid teeth.
SEX
Ovoid teeth are more feminine & square teeth are more masculine; likewise a
curved labial surface is more feminine & a flat labial surface is more
masculine.
51.
AGE
As the featureschange with the aging process; so does the form of the teeth.
The teeth wear at the incisal edges & interproximal surfaces, the labial
surfaces seem flatter & the outline form appears more square
52.
THE SHADE OFTHE ANTERIOR TEETH
Light is electromagnetic radiation that can be detected by the human eye. The
eye is sensitive to wavelengths from approximately 400 (violet) to 700 nm (dark
red). A specific colour of object is recognised by human eye when that
particular object reflects a specific colour and absorbs all the other colours of
the incident light.
THREE DIMENSIONS OF COLOUR
Hue
Value (Brilliance)
Chroma (saturation)
53.
Hue describes thedominant colour of an object such as red, green or yellow.
It is basically the colour of an object. The hue of teeth is usually in the
yellow range.
54.
Value is thelightness or darkness of a colour, which can be measured
independently of the hue.
For example, the yellow of a lemon is lighter than the red of a cherry. The value
increases as an object becomes light or more nearly white. So, greater the value
greater the lightness.
Chroma represents the degree of saturation of a particular hue or colour of an
object
For example, the yellow colour of a lemon is more intense than that of a banana
which is dull yellow. Similarly, in natural teeth the canine and the incisor might
have the same hue but a different chroma, canine is usually more saturated with
colour hence it has more chroma.
55.
• The skincolour is the best guide of tooth shade: People with fair
complexions generally have a lighter teeth. People with dark complexions
generally have a darker teeth.
• Maxillary central incisors are the lightest teeth in the mouth; maxillary
laterals & mandibular incisors are slightly darker, canines are more
darker.
• Posterior teeth are usually uniform in colour & very slightly lighter than
canines.
• Breaking up the colour of anterior teeth by selecting teeth of different
shades from different sets can create the illusion of greater depth &
naturalness.
• The apparent shade of a tooth is affected by its position in the arch.
56.
Generally, when selectingthe mandibular anterior teeth shade, the same
shade selected for the maxillary anterior teeth may be used, but
• For class a iii patient, more darker mandibular anterior teeth would not
appear to stand out as much as lighter teeth.
• For a class ii patient, lighter shade teeth would be used to create the
illusion the teeth are more anterior than they really are.
57.
• The patientshould be in an upright position.
• The patient’s mouth should not be opened too wide.
• The dentist should never approach the patient with the entire shade guide.
• Hold the shade guide outside the mouth against the skin of the face & also
near the eyes & the hair of the patient.
• Always moisten the shade guide.
• Always place the teeth under consideration in the shade of upper lip in the
position they are to occupy.
• Attempt to look at the face as a whole rather than focus entirely on the teeth.
• Whenever possible select the teeth shade under natural light .
CLINICAL GUIDELINES FOR SHADE SELECTION
58.
• Eyes fatigueto color perception very rapidly, there are several ways to help
compensate for this physiologic weakness:
1. Looking steadily at a soft blue, grey or green card before looking at the
shade guide.
2. Place different shade guide teeth in rapid succession in & out of the
mouth & go by the first impression of which is the best mach.
3. The squint test.
• When in doubt about a particular shade, Remember that, the lighter the shade
the more artificial the tooth looks.
• Patient participation in shade selection can be a very delicate matter.
• Remember that the apparent shade of a tooth is affected by its position in the
arch.
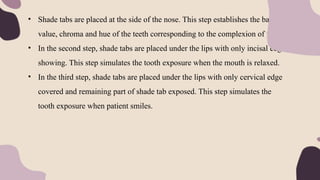
59.
• Shade tabsare placed at the side of the nose. This step establishes the basic
value, chroma and hue of the teeth corresponding to the complexion of face.
• In the second step, shade tabs are placed under the lips with only incisal edge
showing. This step simulates the tooth exposure when the mouth is relaxed.
• In the third step, shade tabs are placed under the lips with only cervical edge
covered and remaining part of shade tab exposed. This step simulates the
tooth exposure when patient smiles.
60.
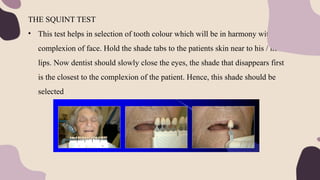
THE SQUINT TEST
•This test helps in selection of tooth colour which will be in harmony with
complexion of face. Hold the shade tabs to the patients skin near to his / her
lips. Now dentist should slowly close the eyes, the shade that disappears first
is the closest to the complexion of the patient. Hence, this shade should be
selected
61.
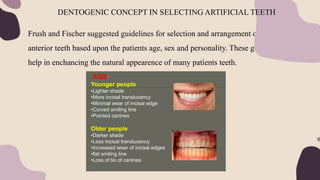
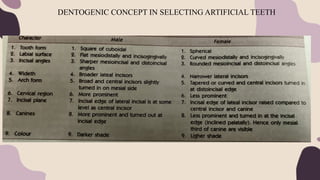
Frush and Fischersuggested guidelines for selection and arrangement of
anterior teeth based upon the patients age, sex and personality. These guidelines
help in enchancing the natural appearence of many patients teeth.
DENTOGENIC CONCEPT IN SELECTING ARTIFICIAL TEETH
Personality:
• Delicate personality:Delicate personality is fragile and frail. Round, light
coloured femine looking teeth are selected for this personality.
• Vigorous personality: This personality is hard and aggressive. Broad teeth
with sharp angles and dark coloured teeth with masculine characters are
selected for this personality.
• Medium personality: This personality is moderate and somewhat robust.
Majority people have medium personality. Teeth with medium characters are
selected (blend of vigorous and delicate characters) for this personality.
64.
The selection ofposterior teeth will be considered in relation to:
1.Shade.
2.Size
3.Form.
4.Material.
POSTERIOR TEETH SELECTION
65.
Shade.
• The shadeof posterior teeth should harmonize with the shade of the anterior
teeth.
• The maxillary premolars may be slightly lighter than the other posterior
teeth, but not lighter than the anterior teeth.
66.
Size & number.The space available for posterior teeth may be defined in three
dimensions:
BUCCOLINGUAL DIMENSION.
• It is desirable to have the bucco-lingual width of the artificial teeth less than
that of the natural teeth.
• This will decrease stresses transferred to the denture supporting area,
increase tongue space, & allow for improved contouring of the polished
surface of the lingual denture flange.
67.
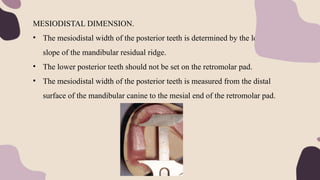
MESIODISTAL DIMENSION.
• Themesiodistal width of the posterior teeth is determined by the length &
slope of the mandibular residual ridge.
• The lower posterior teeth should not be set on the retromolar pad.
• The mesiodistal width of the posterior teeth is measured from the distal
surface of the mandibular canine to the mesial end of the retromolar pad.
68.
OCCLUSO-GINGIVAL DIMENSION.
• Thelength of posterior teeth is determined by the amount of interarch
distance.
• The longer teeth which can be used are more esthetically pleasing than short
teeth specially for the upper premolars (to be esthically in harmony with the
canine).
• Most manufacturers supply posterior teeth in L (long), M (medium) and S
(short) length.
• For patients with minimal interarch space, short bite teeth can be used which
have long facial surfaces but short occlusal portions.
69.
Posterior teeth selection
FORMOF POSTERIOR TEETH
There are three basic tooth moulds:
A. Anatomic.
B. Semi anatomic.
C. Non anatomic.
70.
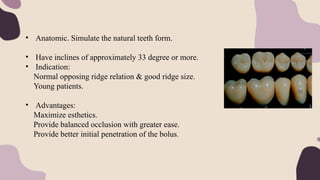
• Anatomic. Simulatethe natural teeth form.
• Have inclines of approximately 33 degree or more.
• Indication:
Normal opposing ridge relation & good ridge size.
Young patients.
• Advantages:
Maximize esthetics.
Provide balanced occlusion with greater ease.
Provide better initial penetration of the bolus.
71.
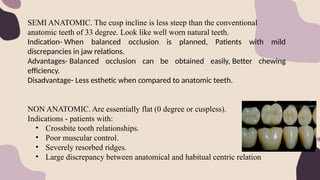
SEMI ANATOMIC. Thecusp incline is less steep than the conventional
anatomic teeth of 33 degree. Look like well worn natural teeth.
Indication- When balanced occlusion is planned, Patients with mild
discrepancies in jaw relations.
Advantages- Balanced occlusion can be obtained easily, Better chewing
efficiency.
Disadvantage- Less esthetic when compared to anatomic teeth.
NON ANATOMIC. Are essentially flat (0 degree or cuspless).
Indications - patients with:
• Crossbite tooth relationships.
• Poor muscular control.
• Severely resorbed ridges.
• Large discrepancy between anatomical and habitual centric relation
72.
Factors in consideration:
1.Ridgemorphology: for broad, well formed ridges, cusped teeth can be used.
2. Inter-arch distance: the more the bone resorption that has taken place, the
greater is the indication for a flat type of tooth morphology.
3. Arch relationship: the class i jaw relationship permits the selection of any
posterior mould but for class ii & iii the patient may do better with the non-
anatomic tooth form.
4. Neuromuscular control: if the muscle control of the patient is questioned,
non-anatomic teeth are indicated.
5. Esthetics: if the patient is extremely concerned about esthetics, anatomic or
semi-anatomic teeth are indicated.
73.
6. Comminution offood: the anatomic teeth are more efficient in masticating
but at the expense of increased horizontal pressure. the efficiency of non-
anatomic teeth can be improved by proper occlusal design . They produce a
lesser horizontal force with a decrease in vertical force.
7. Previous denture wearing experience: they should carefully examined in
relation to wear, occlusal harmony, comfort & efficiency.
In summary, the factor with the greatest input into the choice of anatomic
teeth is the contour of the residual ridge.
74.
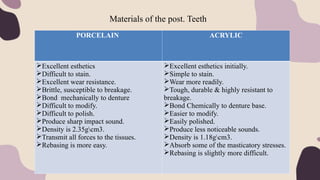
Materials of thepost. Teeth
PORCELAIN ACRYLIC
Excellent esthetics
Difficult to stain.
Excellent wear resistance.
Brittle, susceptible to breakage.
Bond mechanically to denture
Difficult to modify.
Difficult to polish.
Produce sharp impact sound.
Density is 2.35gcm3.
Transmit all forces to the tissues.
Rebasing is more easy.
Excellent esthetics initially.
Simple to stain.
Wear more readily.
Tough, durable & highly resistant to
breakage.
Bond Chemically to denture base.
Easier to modify.
Easily polished.
Produce less noticeable sounds.
Density is 1.18gcm3.
Absorb some of the masticatory stresses.
Rebasing is slightly more difficult.
75.
Materials of thepost. Teeth
Interpenetrating Polymer Network (IPN) Acrylic Resin Teeth.
• To overcome the drawbacks of conventional acrylic resin teeth like
excessive wear, the interpenetrating polymer network (IPN) acrylic resin
teeth were developed.
• This tooth material is a non filled, highly cross linked copolymer with an
interpenetrating polymer network.
• Advantages- More harder, More abrasion resistant, More stain resistant,
More heat resistant.
Composite
• They bond chemically to acrylic denture bases, more esthetic and have
greater wear resistance than conventional acrylic resin teeth.
76.
Materials of thepost. Teeth
Porcelain Acrylic Combination Scheme
• The main disadvantages of porcelain teeth is that they produce clicking
noise in function. To overcome this, a porcelain acrylic combination
scheme was propsed.
• On this scheme, porcelain posterior teeth oppose the acrylic posterior
teeth. This reduces the clicking sound as acrylic teeth act as cushion and
absorbs stresses produced when porcelain teeth occlude with acrylic teeth.
Acrylic Teeth with Amalgam Inserts
• Amalgam inserts also known as amalgam stops are placed in acrylic teeth
to reduce the wear of resin teeth when porcelain teeth are placed in
opposing arch (combination scheme).
• Cavities are prepared in the acrylic resin teeth on occlusal surfaces and
amalgam is condensed into prepared cavities.
77.
Posterior teeth selection
Materialsof the posterior Upper and lower teeth can be
• Both porcelain
• Both acrylic resin.
• A combination of porcelain and acrylic resin teeth, e.g. : resin anterior
teeth & porcelain posterior teeth.
BUT
Resin posterior teeth with porcelain anterior teeth is contraindicated because the
resin teeth will wear rapidly resulting in anterior occlusal discrepancies which in
turn cause destruction of the underlying tissues.
78.
TEETH ARRANGEMENT
• Teetharrangement can be defined as placement of teeth on trial denture bases
for aesthetics, phonetics and function.
• OBJECTIVE
1. To provide a comfortable and atraumatic occlusion.
2. To assist in preparing food for deglutition.
3. To impart a pleasing and natural appearance.
4. To assist in speech.
86.
•A teeth arrangementthat is too perfect may not be ideal. In fact, slight modifications such as
overlapping, tilting, rotation and incisal variations may contribute to a natural looking
denture.
•Use an eccentric midline.
•Place one maxillary central incisor in an anterior direction to the other central incisor.
•Create asymmetry for the maxillary right and left cuspids. Rotate one in posterior direction
than the other.
•Gingival tissues recedes with age. Selecting a long tooth, contouring the wax to show
gingival recession and then staining a bit, can give a natural appearance
87.
•Grinding the incisaledges. Teeth abrade with age. Reshaping the incisal edges and
mesiodistal diameter makes it possible to modify any tooth to desired form.
•Create asymmetry for the maxillary right and left cuspids also helps like rotating one in
posterior direction as compared with the other.
•A hair line crack can be given in the teeth. Silver filling can be given on the posterior teeth.
Cast crown can be given on posterior teeth.. A discolored teeth (as RCT treated) can be
shown by selecting one or teeth of darker shade.
•Spacing and diastema should be given whenever possible between lateral incisor and
cuspid.