

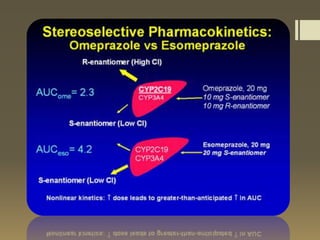


Esomeprazole is the most advanced PPI for acid regulation. It is more effective than omeprazole at reducing acid production due to higher bioavailability from less first-pass metabolism. Esomeprazole has indications for treating GERD, dyspepsia, H. pylori infection, erosive esophagitis, NSAID-induced ulcers, and pathological hypersecretory conditions. It has typical PPI side effects like diarrhea and headaches. Esomeprazole has drug-drug interactions and its dosage depends on the condition being treated, ranging from once daily for GERD to twice daily for Zollinger-Ellison syndrome.










































![hyperacidity_2025[1].pptx readdddddddddddd](https://cdn.slidesharecdn.com/ss_thumbnails/hyperacidity20251-250911140808-bb9b46f0-thumbnail.jpg?width=640&height=640&fit=bounds)
























