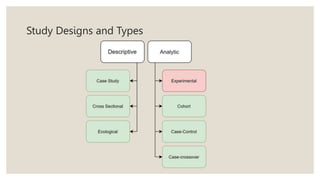
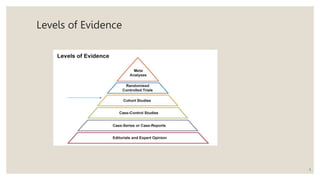
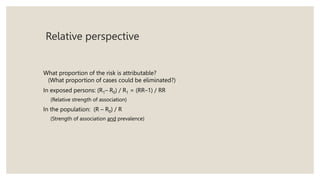
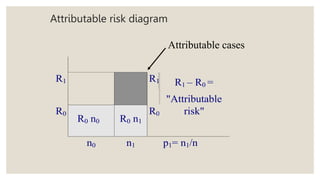
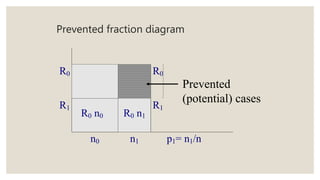
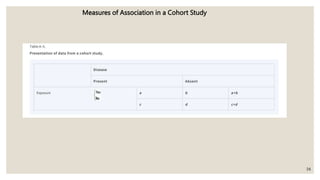
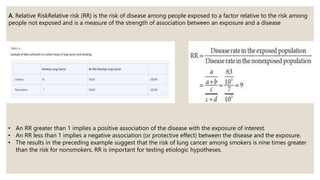
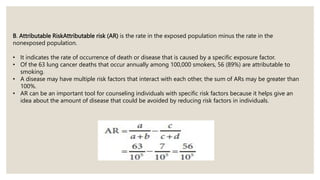
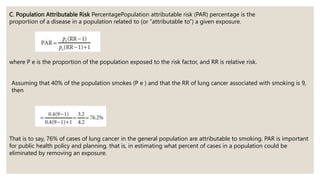
This document outlines cohort studies as a fundamental epidemiological study design for assessing disease incidence and risk factors. It describes the different types of cohort studies, including prospective and historical approaches, and explains measures of association such as relative risk and attributable risk. The importance of these studies in public health and their application in investigating associations between exposures and diseases is emphasized.