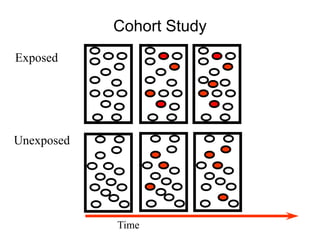
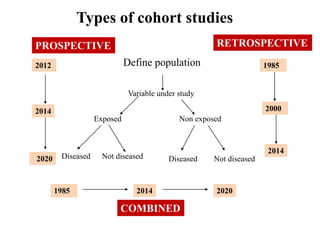
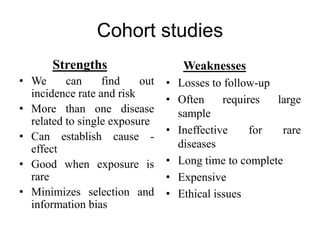
This document discusses cohort studies, including definitions, key elements, types, examples, strengths, and weaknesses. A cohort study examines groups of individuals who are alike in many ways but differ by a certain characteristic (e.g. exposure to a risk factor) and follows them over time to determine outcomes. Key elements include selection of study subjects, obtaining exposure data, follow up, and analysis. The Framingham Heart Study is highlighted as a landmark prospective cohort study that identified many risk factors for cardiovascular disease.



































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








