Downloaded 11 times


![CONCLUSION
The study showed that through small adjustments
better patient adherence can be achieved especially in
the warm South African climate.
System B demonstrated an improved patient
adherence due to the wash ability and aeration of the
cast material
It is recommended that more skills training
workshops are needed in order to guide health
professionals and change perceptions in incorporating
TCC as the gold standard in all practices working
with patients with diabetic foot ulcers.
Howard Alexander
www.fixmyfeet.biz
howardal@mweb.co.za
Liezl Naude
www.eloquent.co.za
Liezl@eloquent.co.za
EWMA 2014 EP495
5
1. Sinacore, D.R., Mueller, M.J.,. Off-loading for diabetic foot disease. [book auth.] Pfeifer M.A., Bowker J.H. Levin and O'Neal'sThe Diabetic Foot. Philadelphia : Mosby Elsevier, 2008, 13, pp. 287-
304.
2. Wounds International. International Best Practice Guidelines:Wound Management in Diabetic Foot Ulcers. International Best Practice Guidelines:Wound Management in Diabetic Foot Ulcers.
London :Wounds International, 2013.Available from: www.woundsinternational.com.
3. Current concepts in offloading diabetic foot ulcers. Fitzgerald R.H. 9, 2009, PodiatryToday,Vol. 22, pp. 16-21.
4. Foot ulcers in the diabetic patient, prevention and treatment. Wu S.C., DriverV.R.,Wrobel J.S.,Armstrong D.G.,. 1, 2007,Vasc Health Risk Manag,Vol. 3, pp. 65-76.
5. Podiatric intervention in the management of a diabetic foot ulceration: a case study using total contact casting. F.J., Howard. 2, s.l. : Medpharm Publications, 2012,Wound Healing Souther Africa,Vol. 5,
pp. 96-101.
6. Cavanagh P.R., Ulbrecht J.S.,. The biomechanics of the foot in diabetes mellitus. [book auth.] Pfeifer M.A., Bowker J.H. Levin and O'Neal's the Diabetic Foot. Philadelphia : Mosby Elsevier,
2008, pp. 115-184.
7. Armstrong D.G., Bevilacqua N.J.,Wu S.C.,. Offloading foot wounds in people with diabetes. [book auth.] Rodeheaver G.T., Sibbald R.G., Krasner D.L. ChronicWound Care: a clinical source
book for healthcare professionals. 4th edition. Malvern : HMP Communications, 2007, pp. 557-563.
8. Effectiveness and saftey of a fiberglass offbearing cast versus a therapeutic shoe in the treatment of neuropathic foot ulcers. Caravaggi C., Faglia E., De Gigglio R., et al,. 12, 2000, Diabetes Care,
Vol. 23, pp. 1746-1751.
9. What are the most effective interventions in preventing diabetic foot ulcers? Lavery L.A., Peters E.J.G.,Armstrong D.G.,. 1, 2008, International Wound Journal,Vol. 1, pp. 425-433.
10. Orsted H.L., Inlow S.,. The team approach to treating ulcers in people with diabetes. [book auth.] Rodeheaver G.T., Sibbald R.G., Krasner D.L. Chronic wound care: a clinical source book for
healthcare professionals. 4th edition. Malvern : HMP Communications, 2007, pp. 565-571.
11. Krasner D.L., Rodeheaver G.T., Sibbald R.G.,. Inter-professional wound care. Chronic wound care: a clinical source book for healthcare professionals, 4th edition. Malvern : HMP
Communications, 2007, pp. 3-11.
12. Kenshole A.B., Macdonald J.,. The role of the healthcare team in the prevention and management of diabetic foot ulcers. [book auth.] Rodeheaver G.T., Sibbald R.G., Krasner D.L. Chronic
wound care: a clinical source book for healthcare professionals 4th edition. Malvern : HMP Communications, 2007, pp. 543-547.
13. Principles of management of vascular problems in the diabetic foot. Tudhope L. 2, s.l. : CME, 2010,Vol. 28, pp. 158-163.
14. Landis S., Ryan S.,Woo K., Sibbald R.G.,. Infections in chronic wounds. [book auth.] Rodeheaver G.T., Sibbald R.G., Krasner D.L. Chronic wound care: a clinical source book for healthcare
professionals. 4th edition. Malvern : HMP Communications, 2007, pp. 299-321
REFERENCES](https://image.slidesharecdn.com/ep495457-140814090513-phpapp01/85/EWMA-2014-EP495-TOTAL-CONTACT-CASTING-A-SOUTH-AFRICAN-APPROACH-TOWARDS-OFFLOADING-THE-DIABETIC-FOOT-5-320.jpg)

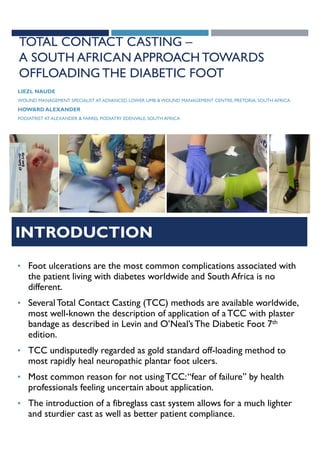
This study evaluated two total contact casting (TCC) systems for offloading diabetic foot ulcers and stabilizing Charcot feet in South Africa. System B, which used a washable, water resistant inner lining, demonstrated better patient adherence and aeration compared to System A. Both systems effectively reduced plantar pressures and healed wounds within 36 days on average. The study concluded that TCC is the gold standard for offloading but more training is needed for healthcare professionals to incorporate it widely in practice.






















































































