Download to read offline
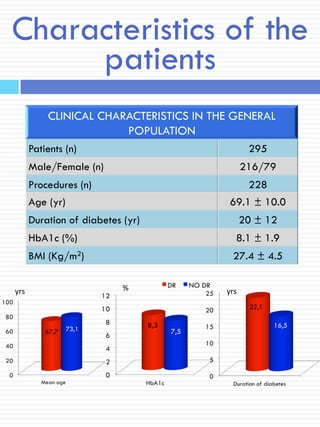



The study evaluated the prevalence of diabetic retinopathy (DR) in 295 type 2 diabetic patients with diabetic foot complications and found that 70% exhibited some degree of DR. A correlation was observed between the severity of DR and the severity of peripheral arterial disease (PAD), although no correlation was established with age, duration of diabetes, or HbA1c levels. The findings suggest a significant relationship between DR and PAD in this patient population.



































































