
Download as PDF, PPTX
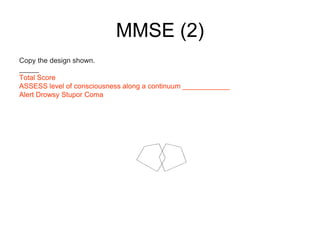
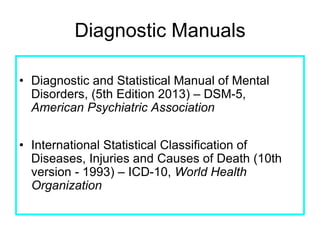
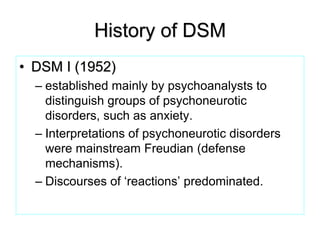
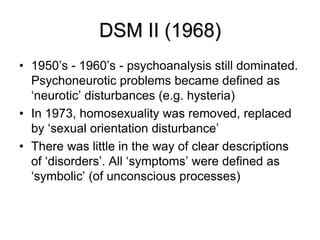
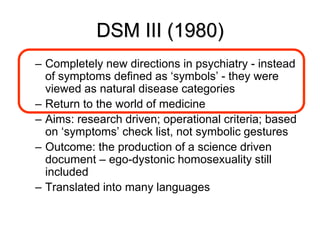

This document discusses the classification of mental disorders and the process of psychiatric assessment. It provides an overview of the purpose of diagnosis in psychiatry, including establishing order and structure, facilitating communication, predicting outcomes, deciding on appropriate treatment, and assisting research. It then describes the typical procedures for clinical assessment, including using clinical interviews as the primary assessment tool. It outlines various assessments used, including psychological tests and biological measures. It details the typical components of a psychiatric assessment, such as identifying data, chief complaint, history, mental status exam, and diagnosis. Finally, it discusses several assessment tools and rating scales, including the Mini-Mental State Examination and Positive and Negative Syndrome Scale.
























![1 1 definition, methode and scope [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1definitionmethodeandscopecompatibilitymode-151003100439-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)







































