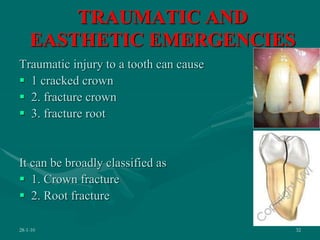
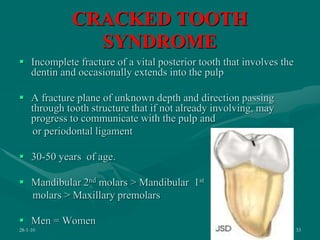
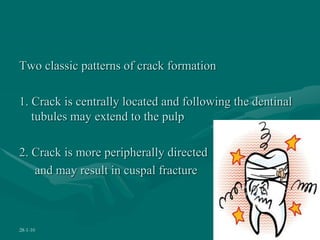
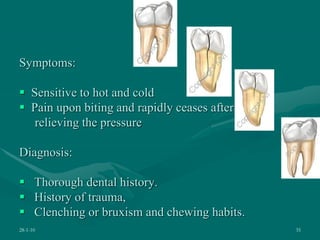
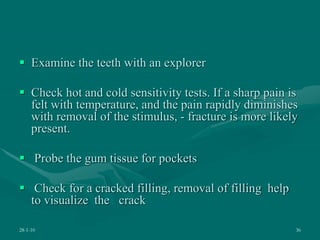
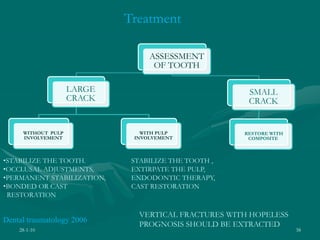
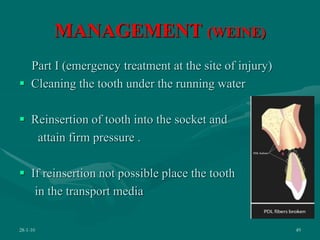
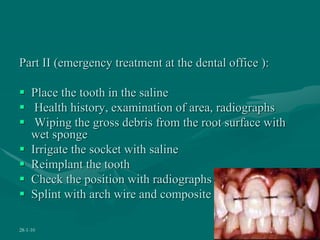
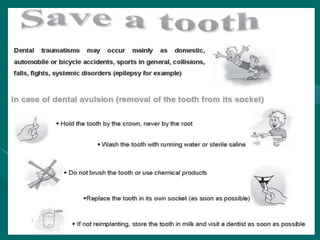
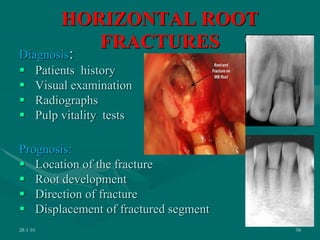
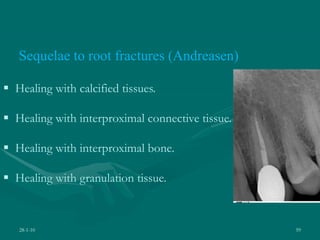
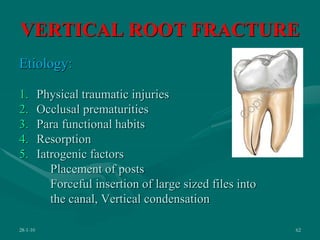
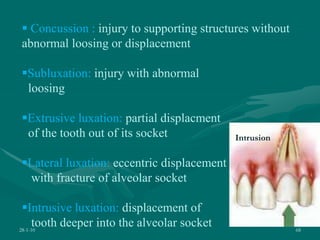
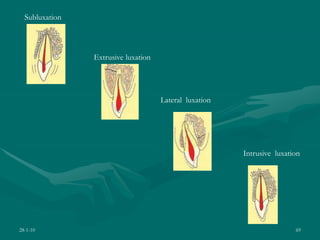
The document discusses various endodontic emergencies including their causes, symptoms, diagnosis and treatment. It defines an endodontic emergency as an unscheduled visit associated with pain or swelling from pulpoperiapical pathoses requiring immediate treatment. Common endodontic emergencies include acute pulpitis, acute apical abscess, cracked tooth syndrome, tooth fractures, and tooth avulsion. The document provides details on diagnosing and managing each emergency through methods like pulpectomy, apical trephination, incision and drainage, splinting or reimplantation depending on the specific emergency.